
Hey there, let’s get straight to the point: Yes, it is possible to have both lymphoma and leukemia at the same time, but it’s extremely rare. Most people hear the names and assume they’re interchangeable cousins, yet the reality is more nuanced. In the next few minutes, I’ll walk you through what these cancers are, why they sometimes overlap, what the symptoms look like, and what you can actually do if you—or someone you love—faces a dual diagnosis. Grab a cup of tea, settle in, and let’s unravel this together.
What Are Both?
Understanding the basics
Lymphoma and leukemia are both types of blood cancer, but they start in different neighborhoods of your body. Leukemia usually begins in the bone marrow—the spongy, blood‑producing tissue inside your bones. The rogue cells then spill out into the bloodstream, crowding out healthy blood cells.
Lymphoma, on the other hand, originates in the lymphatic system—think of it as the body’s drainage network of nodes, vessels, spleen, and tonsils. Instead of drifting freely through the blood, the malignant cells tend to clump together and form tumors in lymph nodes or related tissue.
How can they appear together?
The phrase “both lymphoma and leukemia” usually describes one of three scenarios:
- A true dual diagnosis where two separate cancers are discovered at the same time.
- A transformation, such as Richter’s syndrome, where chronic lymphocytic leukemia (CLL) morphs into an aggressive form of lymphoma.
- A therapy‑related second cancer that shows up years after treatment for the first cancer, often because chemotherapy or radiation can damage healthy cells.
Regardless of the route, the key takeaway is that the two diseases share a common lineage—abnormal white blood cells—yet they usually stay in their own lanes. When they cross, it’s a sign that the disease is behaving unusually, and extra vigilance is needed.
How They Differ
Origin and cell type
Leukemia starts in the bone marrow and can be classified as myeloid or lymphoid depending on the type of blood cell that goes rogue. Lymphoma begins in the lymphatic system and is usually categorized as Hodgkin or non‑Hodgkin. Below is a quick visual snapshot:
| Feature | Leukemia | Lymphoma |
|---|---|---|
| Primary site | Bone marrow → bloodstream | Lymph nodes & lymphatic tissue |
| Typical cells | Myeloid or lymphoid white blood cells | Lymphocytes (B‑cells or T‑cells) |
| Common types | ALL, AML, CLL, CML | Hodgkin, Non‑Hodgkin ( >70 subtypes) |
| Age groups | ALL: children; CLL: adults >60 | Hodgkin: teens‑20s; Non‑Hodgkin: all ages |
Symptoms – what overlaps, what’s unique?
Both cancers can cause fatigue, fever, night sweats, and unexplained weight loss—the dreaded “B‑symptoms.” However, there are a few clues that tip the scales toward one or the other:
- Lymphoma symptoms: Painless, swollen lymph nodes (especially in neck, armpit, or groin), itching skin, and sometimes a visible lump.
- Leukemia symptoms: Frequent bruising or bleeding, pale skin from anemia, bone or joint pain, and infections that won’t clear.
When both sets of signals appear, it’s worth asking your doctor for a thorough work‑up. According to a review by the Cancer Center, “patients who present with both sets of symptoms should be evaluated for a possible transformation or secondary malignancy”[[source]](https://www.cancercenter.com/blood-cancers/leukemia-vs-lymphoma){rel=”nofollow noreferrer” target=”_blank”}.
Dual Diagnosis Paths
Richter’s syndrome
Richter’s syndrome is a rare but well‑documented phenomenon where CLL—usually an indolent, slowly progressing leukemia—suddenly morphs into an aggressive non‑Hodgkin lymphoma. It occurs in roughly 2‑10 % of CLL patients. The change can happen without a clear warning, which is why routine monitoring is critical.
Treatment‑induced second cancers
Radiation and certain chemotherapy agents wield a double‑edged sword. While they can eradicate the first cancer, they may also cause DNA damage in healthy cells, setting the stage for a second malignancy later on. For instance, survivors of Hodgkin lymphoma have a higher risk of developing acute myeloid leukemia (AML) years after their initial treatment.
Genetic and molecular overlap
On a microscopic level, both diseases can share genetic mutations—like the MYC or BCL2 translocations—that drive uncontrolled cell growth. Leading researchers, such as Dr. Dinesh Rao at UCLA, emphasize that “understanding these shared pathways is key to developing targeted therapies that can tackle both diseases simultaneously”[[source]](https://medschool.ucla.edu/news-article/leukemia-vs-lymphoma-what-is-the-difference){rel=”nofollow noreferrer” target=”_blank”}.
How It’s Diagnosed
Blood work and bone‑marrow biopsy
First, doctors will order a complete blood count (CBC) to look for abnormal white‑cell counts, anemia, or low platelets. If something feels off, a bone‑marrow aspiration/biopsy follows, letting pathologists examine the cells under a microscope.
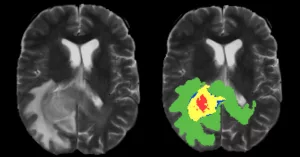
Imaging and PET‑CT
For lymphoma, imaging tests like CT scans, MRI, or a PET‑CT are essential to locate swollen nodes and gauge how much disease is present. PET‑CT is also valuable for detecting hidden leukemia cells that have migrated to lymph nodes.
Molecular testing
Flow cytometry, fluorescence in‑situ hybridization (FISH), and next‑generation sequencing (NGS) help pinpoint specific genetic abnormalities. Knowing the exact mutation often guides whether targeted drugs—like ibrutinib for CLL or pembrolizumab for certain lymphomas—are appropriate.
Treatment Options
Standard therapies
Both cancers are treated with chemotherapy, but the drug mixtures differ. Leukemia may need agents like cytarabine or anthracyclines, while lymphoma protocols often include CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone) or ABVD for Hodgkin disease.
Integrated plans for dual disease
When both cancers coexist, oncologists craft a tailored plan that addresses the most aggressive component first. For example, with Richter’s syndrome, lymphoma‑directed therapy (often immunochemotherapy) takes precedence because it progresses quickly.
Decision‑tree snapshot
- If CLL is stable and lymphoma appears, start lymphoma treatment.
- If acute leukemia is the dominant issue, prioritize intensive chemotherapy or stem‑cell transplant, then reassess lymphoma status.
- Consider clinical trials that explore combined regimens—many are enrolling patients with mixed blood‑cancer profiles.
Emerging therapies
CAR‑T cell therapy, which re‑engineers a patient’s own T‑cells to hunt cancer, has shown promise for both relapsed ALL and certain aggressive lymphomas. Stem‑cell transplantation remains a curative option for many younger patients, especially when the disease is caught early.
Risks & Benefits of Knowing
Early detection saves lives
Finding a second cancer early dramatically improves survival odds. The Cancer Center reports that patients diagnosed with a secondary malignancy within the first two years of their primary cancer had a 30 % higher five‑year survival rate than those diagnosed later.
Potential treatment toxicity
Balancing two treatment regimens can increase side‑effects—like heightened infection risk, organ strain, or fatigue. That’s why multidisciplinary teams (hematology, oncology, cardiology, nutrition) collaborate to monitor organ function and adjust dosing.
Emotional impact
Learning you have “both” can feel like a double punch. It’s normal to experience anxiety, anger, or even denial. Support groups—both online and in‑person—offer a safe space to share fears and coping strategies. Remember, you’re not navigating this alone.
Living With Both
Monitoring symptoms
Keep a symptom diary. Note changes in energy, new bruises, swelling of nodes, fevers, or unexpected weight loss. Share this log with your care team at each appointment—early tweaks can prevent major setbacks.
Nutrition, exercise, and weight
Maintaining a healthy BMI (under 30) lowers the risk of many cancers, including both lymphoma and leukemia, according to Healthline. Simple lifestyle steps make a difference:
- Eat a rainbow of vegetables and lean proteins.
- Aim for at least 150 minutes of moderate activity each week—walking, swimming, or gentle yoga works well.
- Stay hydrated and limit alcohol intake.
Financial and insurance navigation
Medical costs can be overwhelming. Consider these resources:
- The American Cancer Society’s financial assistance program.
- Local non‑profits that provide co‑pay help for chemotherapy.
- Hospital social workers—most major cancer centers have them on staff.
Conclusion
So, can you have both lymphoma and leukemia? Absolutely—but it’s a rare and complex scenario that requires vigilant monitoring, expert medical guidance, and a solid support network. Understanding the differences, recognizing overlapping symptoms, and knowing the paths that lead to a dual diagnosis give you power over an otherwise frightening prospect. If you or a loved one are facing this journey, stay proactive, ask questions, and never hesitate to lean on the expertise of your care team.
We’ve covered a lot today, from the science behind these blood cancers to practical steps you can take right now. I hope you feel more informed and a bit less alone. If you have any thoughts, experiences, or questions, please share them below—your story could help someone else feel less isolated.




















Leave a Reply
You must be logged in to post a comment.