
Imagine your little one suddenly seems wired, loses weight even though they’re “hungry all the time,” and can’t sit still in class. It can feel like you’ve stepped onto a roller‑coaster you never signed up for. That’s often the first hint of hyperthyroidism in children—a condition where the thyroid gland cranks the body’s metabolism up to eleven. In the next few minutes, I’ll walk you through what it looks like, why it happens, and how you can get it under control, all in plain language and with a dash of friendly empathy.
What Is It?
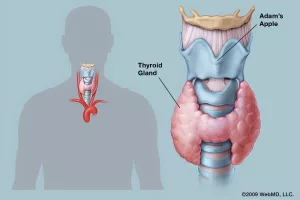
Hyperthyroidism means the thyroid—a butterfly‑shaped gland in the neck—produces too much thyroid hormone. In kids, this excess hormone (known as thyroid hormone excess) speeds up almost every bodily function: heart beats faster, the body burns more calories, and the brain can feel overstimulated.
Why It Matters
Getting a handle on this early can be a game‑changer. Proper treatment lets kids grow, learn, and play without the constant “on‑high‑alert” feeling. Left unchecked, the excess hormone can sabotage growth, shake the heart, and even spark a life‑threatening thyroid storm. Think of it as a balance beam—tipping too far one way makes everything wobble; finding the center brings stability.
Quick Stats
- Children make up only about 1‑5 % of all hyperthyroidism cases, but the condition is three‑times more common in girls than boys.
- Graves’ disease accounts for roughly 95 % of pediatric cases.
- Most diagnoses happen between ages 10‑15, though it can appear earlier.
These numbers come from the American Thyroid Association’s patient brochure and the Merck Manual’s recent update (according to the ATA).
Spotting the Signs
Infants & Toddlers
Little bodies can’t always explain what’s wrong, so watch for:
- Rapid, unexplained weight loss despite a good appetite
- Persistent irritability or crying that “won’t calm down”
- Fever‑ish feeling, sweating, or warm skin
- Fast heart rate (you might feel a flutter when you place your hand on their chest)
- Enlarged fontanelle or a noticeable swelling at the base of the neck
School‑Age Children
When kids start school, the clues shift toward behavior and performance:
- Difficulty concentrating, often mistaken for attention‑deficit traits
- Sudden drop in grades or school participation
- Weight loss with a ravenous appetite
- Frequent bowel movements or diarrhea
- Tremors—shaky hands when they try to write or hold a fork
- Feeling hot or sweaty even when others are comfortable
- Heart palpitations (“my heart feels like it’s racing”)
Teenagers
Teens may show classic adult‑type clues, plus a few extra:
- Bulging eyes (a hallmark of Graves’ disease)
- Visible goiter—an enlarged thyroid that looks like a small bump in the throat
- Irregular menstrual cycles in girls
- Shiny, smooth skin or unexpected hair loss
- Restlessness and a “can’t sit still” vibe
Symptom Checklist (Table)
| Symptom | Typical Age | Why It Happens |
|---|---|---|
| Rapid heartbeat | All | ↑ β‑adrenergic activity from excess hormone |
| Weight loss | All | Higher basal metabolic rate burns calories faster |
| Sleep trouble | All | Hormone over‑stimulation of the CNS |
| Heat intolerance | All | Thermoregulation ramps up |
| Bulging eyes | Teens | Autoimmune inflammation behind the eyes |
What Causes It?
Graves’ Disease – The Usual Suspect
Think of Graves’ disease as the body’s misguided “cheerleader” that shouts “Go, thyroid, go!” ALL the time. The immune system creates an antibody (TSI) that binds to the thyroid‑stimulating hormone receptor, forcing the gland to crank out extra hormone. This accounts for ~95 % of pediatric cases.
Other, Less‑Common Triggers
- Autonomous (“hot”) nodules: A single thyroid growth that produces hormone on its own.
- Thyroiditis: Inflammation (often viral) releases stored hormone; the condition is usually self‑limited.
- Medication‑induced: Excess levothyroxine or drugs like amiodarone can tip the balance.
- Neonatal Graves’: Mother’s antibodies cross the placenta, causing temporary excess in newborns.
Risk Factors
Family history matters—a sibling or parent with an autoimmune disease (type 1 diabetes, celiac, Hashimoto thyroiditis) ups the odds. Girls are more susceptible, especially during puberty, and environmental triggers (stress, infections) can play a role.
How Doctors Diagnose It
Clinical Evaluation
The doctor will check for a goiter, rapid pulse, and eye changes, then chart growth curves to see if the child is outpacing or lagging behind typical patterns.
Blood Tests – The Core Panel
- Free T4 & Free T3 – usually high.
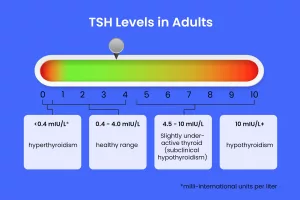
- TSH – suppressed (low) because the pituitary senses excess hormone.
- TSI/TSHR‑Ab – positive in Graves’ disease.
- Baseline liver and blood counts before starting medication.
Imaging When Needed
Ultrasound helps spot nodules; a radioactive iodine uptake scan tells whether the whole gland is overactive (diffuse) or just a spot (focal).
Diagnostic Flowchart (Quick Reference)
- Identify symptoms →
- Order thyroid panel →
- Check antibodies →
- If unclear, add ultrasound or scan →
- Confirm diagnosis and decide on treatment.
Treatment Options – What Works Best?
First‑Line: Antithyroid Medications
Methimazole is the go‑to drug for most kids. It blocks hormone production and usually steadies levels within weeks. Propylthiouracil (PTU) is reserved for early pregnancy or specific situations because of liver‑related risks.
Beta‑Blockers for Symptom Relief
Propranolol (or another beta‑blocker) tames heart palpitations, tremors, and anxiety while the antithyroid meds take effect.
Definitive Therapies
| Modality | When Considered | Pros | Cons |
|---|---|---|---|
| Radioactive Iodine (RAI) | Kids ≥5 yr, stable, no pregnancy | Outpatient, permanent cure | Often leads to lifelong levothyroxine, needs isolation precautions |
| Surgical Thyroidectomy | Large goiter, cancer suspicion, RAI contraindicated | Immediate control, no radiation | Risk of vocal‑cord injury, hypoparathyroidism |
| Observation | Transient thyroiditis | Avoids meds | Requires close monitoring for relapse |
Dr. Sobenna George of Children’s Healthcare of Atlanta explains that “a nodule that’s overproducing hormone often needs surgery, while most Graves’ cases respond well to medication or later RAI” (according to CHOA).
Real‑World Example
Take 12‑year‑old Maya. She started losing weight rapidly and her school grades dropped. Blood work showed a high free T4 and a suppressed TSH; antibodies were positive for Graves’. After six weeks of methimazole, her heart rate normalized, she stopped feeling “wired,” and her grades improved. Two years later, her endocrinologist recommended a low‑dose RAI to cement the cure. Maya’s story illustrates how medication can bridge the gap to a lasting solution.
Living With Hyperthyroidism
Daily Management Tips
- Take medication at the same time each day—set a reminder on your phone.
- Keep a symptom diary (pulse, mood, weight) to share at appointments.
- Ask the school for a quiet space during tests if anxiety spikes.
Nutrition & Lifestyle
While there’s no special “thyroid diet,” limiting caffeine (soda, chocolate) can keep the heart from racing. Calcium‑rich foods (milk, yogurt, leafy greens) support bone health, especially if a child will need lifelong thyroid hormone replacement after RAI or surgery.
Emotional Support
Hyperthyroidism can feel like a roller‑coaster of emotions. Encourage open conversations, consider counseling, and let your child know that mood swings are a symptom, not a character flaw. Peer support groups—many hospitals run them online—can also provide a sense of community.
When to Call for Help
If your child develops a fever, severe rapid heartbeat, confusion, or passes out, treat it as an emergency—call 911. These could signal a thyroid storm, which is rare but life‑threatening.
Final Thoughts
Speedy recognition and thoughtful treatment turn a bewildering diagnosis into a manageable chapter of your child’s life. Whether the culprit is Graves’ disease or a solitary “hot” nodule, modern pediatric endocrinology offers medications, radio‑iodine, and surgery—all backed by solid research and compassionate care.
Take heart: with the right plan, most kids regain a normal, energetic childhood, excel in school, and grow into healthy adults. If you notice any of the signs above, schedule an appointment with a pediatric endocrinologist—early action makes all the difference.
What’s your experience with child thyroid symptoms? Share your story in the comments or ask any lingering questions. You’re not alone on this journey, and together we can keep our kids thriving.




















Leave a Reply
You must be logged in to post a comment.