
Chronic obstructive pulmonary disease (COPD) refers to a collection of lung disorders, including chronic bronchitis and emphysema, that obstruct airflow and make breathing difficult.
Modern medicine has clarified what drives these illnesses and has improved approaches to treating them. That wasn’t always the situation.
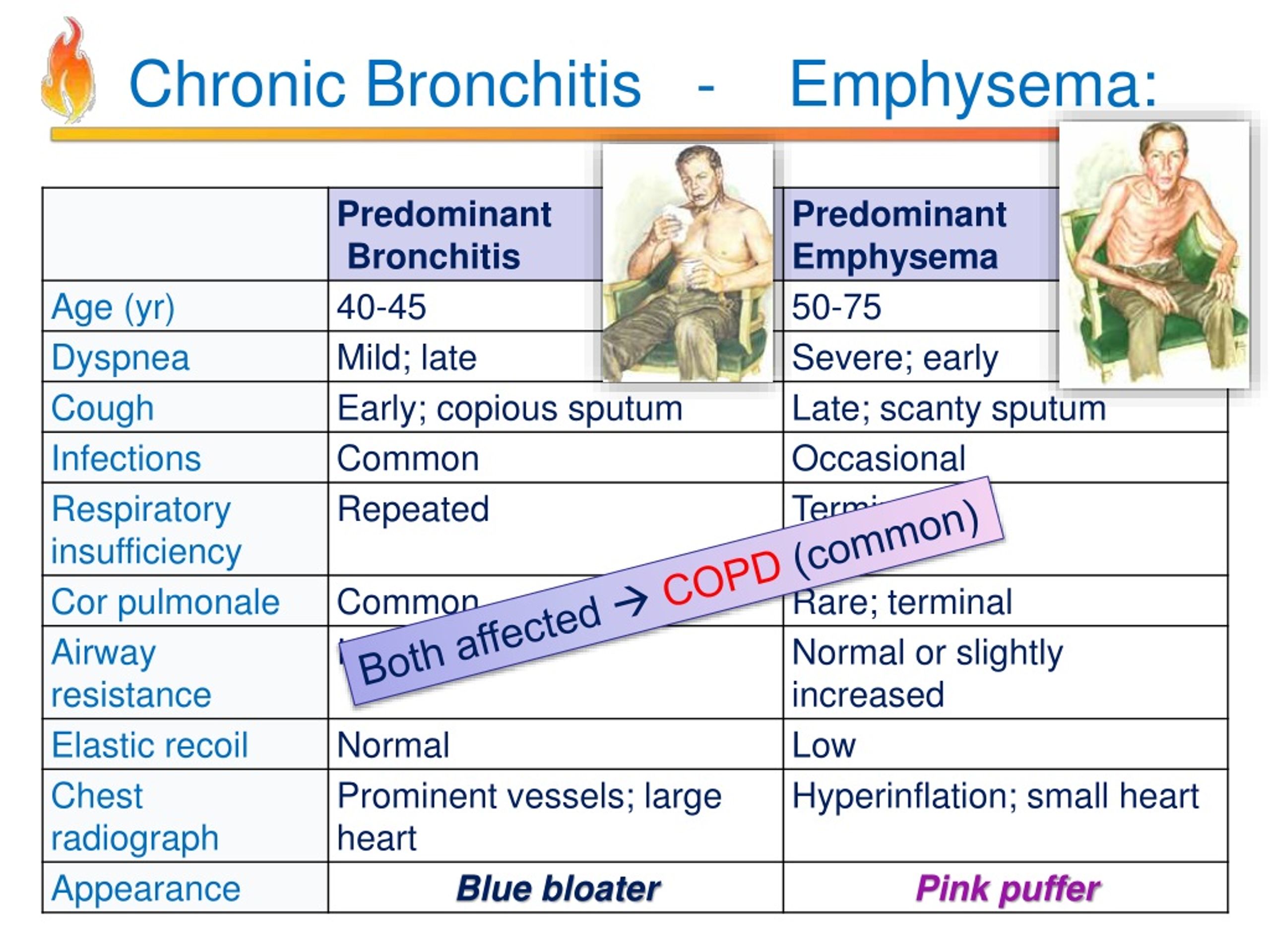
Historically, clinicians used the expressions “blue bloater” and “pink puffer” to categorize types of patients with COPD. These phrases captured stereotyped appearances tied to certain COPD symptoms.
They’re now seen as inaccurate and disrespectful, though you may still encounter them in older medical literature.
What did “blue bloater” mean?
The label “blue bloater” was once applied to patients with chronic bronchitis.
Clinicians called these patients “blue bloaters” because chronic bronchitis can severely impair breathing and lower blood oxygen levels. That may produce a bluish tint to a person’s skin and lips.
Some of these patients were also overweight. People with chronic bronchitis commonly have a persistent cough and may be unable to get adequate oxygen even when taking deep breaths.
What did “pink puffer” mean?
“Pink puffer” was historically used for people with emphysema. The term reflected the breathing pattern of these patients.
Because emphysema makes it hard to catch one’s breath, sufferers often take quick, shallow breaths or pause between inhalations. This can produce a temporary flushed or pink appearance on the face and cheeks.
Why these labels fell out of use
Words matter
Previously, clinicians used pigeonholing words like “blue bloaters” and “pink puffers” to summarize how some people with COPD appeared. Those terms are stigmatizing and insulting, and they’re no longer considered appropriate clinical descriptors.
There are several reasons these expressions have been abandoned.
Chief among them is that the labels were founded on superficial stereotypes of how these illnesses looked. That risked overlooking or misdiagnosing people with milder or atypical presentations.
Such terminology demeans patients and offers little clinical value. It fails to explain the physiological processes underlying a person’s condition.
Today we recognize COPD, chronic bronchitis, and emphysema much more clearly. Clinicians now understand that many people with COPD exhibit features of both chronic bronchitis and emphysema, which makes the old binary of “blue bloater” versus “pink puffer” even less helpful.
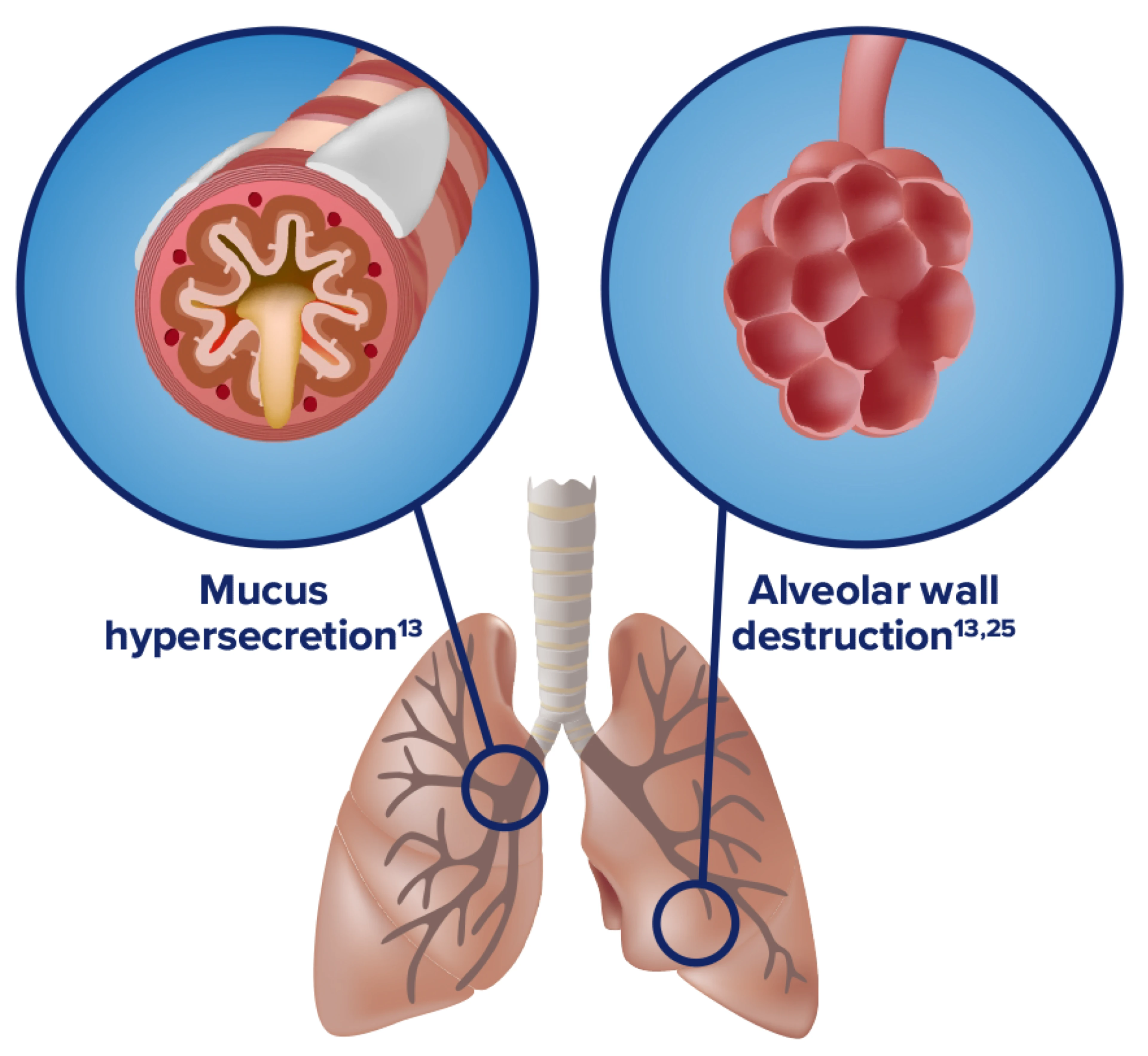
What is chronic bronchitis?
Chronic bronchitis happens when the airways in your lungs become persistently inflamed. The main cause is cigarette smoking, though factors like air pollution and a family history of bronchitis can also contribute.
There’s no cure for chronic bronchitis, but symptoms can be managed with therapies and lifestyle adjustments.
Symptoms
Symptoms of chronic bronchitis can resemble other conditions such as asthma or upper respiratory infections. The disease may evolve slowly. You might have a long-standing cough for years before noticing breathing difficulties or chest tightness.
You should consult a healthcare provider about any cough that lasts more than a week or two.
Typical symptoms include:
- persistent cough
- cough that produces mucus
- wheezing
- chest discomfort or pain
- shortness of breath
Diagnosis
Diagnosing chronic bronchitis begins with a clinical visit. Your clinician will review your symptoms and medical history, with smoking history being particularly relevant. You may require tests to confirm the diagnosis.
The most common diagnostic tools measure lung function, known as pulmonary function tests. These involve breathing into a device that records how well your lungs inhale and exhale.
Other assessments may include X-rays, CT scans, and blood tests.
Read this article for more information about how COPD is diagnosed.
Treatment
Treatment for chronic bronchitis combines lifestyle measures and medical therapies. Your specific plan depends on the severity of your condition and how you respond. Ongoing management may include:
- quitting smoking
- using a humidifier at home
- avoiding airborne irritants and smoke
- taking prescribed oral medications to clear airways
- using inhaled medicines to open airways
- using portable oxygen to maintain adequate oxygen levels
- participating in pulmonary rehabilitation to improve breathing control
Questions to ask your clinician
Receiving a new diagnosis can feel overwhelming, especially for a long-term condition like COPD.
Talking with your clinician about your condition and choices can clarify expectations. Helpful questions include:
- Do I need any further tests?
- How advanced is my COPD?
- Which treatments do you recommend?
- What should I expect from my condition?
- Are there alternative therapies available?
- What actions can I take at home to ease symptoms?
- How might my COPD progress?
- What are the next steps if this treatment is ineffective?
- How can I reduce the chance of COPD flare-ups?
What is emphysema?
Emphysema is a slowly progressive lung disease in which the tiny air sacs (alveoli) in lung tissue are damaged. Over time these structures break down and merge into larger air spaces, trapping air and making breathing more difficult.
Smoking is the primary cause of emphysema, though air pollution and repeated lung infections can also play a role.
Symptoms
Because emphysema advances gradually, many people live with it for years before symptoms appear. Shortness of breath is usually the first sign.
Shortness of breath from emphysema is often mistaken for poor fitness. As the disease worsens, breathing difficulty can happen even at rest.
Diagnosis
At your appointment, your clinician will review your history and symptoms and ask about tobacco exposure. Tests to confirm emphysema often include assessments of lung function.
Pulmonary function tests require you to breathe into a handheld device to measure how much air you can move and how effectively your lungs work. Imaging studies may also be used to view lung structure and exclude other causes of breathlessness.
Treatment
Treatment for emphysema usually combines therapies, medications, and self-care. The best approach depends on disease stage and treatment response. Potential treatments include:
- maintaining a healthy weight
- quitting smoking
- taking prescribed oral medications to clear airways
- using inhaled medications to open airways
- using supplemental oxygen
- attending pulmonary rehabilitation to improve breathing techniques
- surgery to remove severely damaged lung tissue
The bottom line
Historically, clinicians used the phrases “blue bloater” and “pink puffer” to depict types of COPD: “blue bloater” for chronic bronchitis and “pink puffer” for emphysema.
Those terms reflected stereotyped physical traits some people with these diseases displayed. With improved understanding of these conditions, such labels are now viewed as stigmatizing and medically unhelpful.
Today, healthcare professionals prefer to use the specific terms chronic bronchitis and emphysema for clearer, more respectful diagnosis and care.



















Leave a Reply
You must be logged in to post a comment.