
Key takeaways
- Hormone therapies, also referred to as androgen deprivation therapy, help slow tumor progression by reducing hormones such as testosterone, while nonhormone treatments like chemotherapy and radiation are designed to eliminate existing cancer cells.
- Hormone therapy is typically the first-line treatment for advanced prostate cancer. If resistance develops, nonhormone strategies may help delay further spread and prolong survival, although a definitive cure is unlikely.
- Choosing the right treatment involves weighing goals of care, possible side effects, and personal eligibility, in close consultation with an oncologist to design an individualized plan that may combine hormone and nonhormone therapies.

If prostate cancer advances and spreads to distant areas of the body, active treatment becomes necessary. At this stage, watchful waiting — which may have been appropriate earlier — is generally no longer recommended.
Many people searching for answers about Life expectancy after Xtandi fails are facing difficult decisions about next steps. When prostate cancer progresses despite treatment with enzalutamide (Xtandi), understanding the full range of available therapies can provide clarity and hope. Today, individuals with advanced or metastatic prostate cancer have more available treatment options than ever before, including both hormone-based and nonhormone approaches.
The treatment plan recommended for you will depend on the stage of your cancer, whether it has become castration-resistant, and any other health conditions you may have. No two people experience prostate cancer in exactly the same way, so therapy must be tailored to the individual.
When evaluating options, it’s important to consider the overall objective of care — whether that’s extending survival, controlling symptoms, or improving quality of life — along with potential side effects and your candidacy for certain drugs or procedures. Being well informed empowers you and your oncologist to select the most appropriate treatment or combination of treatments.
Hormone therapies for advanced prostate cancer
Hormone therapy, also called androgen deprivation therapy (ADT), remains a cornerstone treatment for metastatic prostate cancer.
How hormone therapy works
Hormone therapy lowers levels of androgens in the body. Androgens, including testosterone and dihydrotestosterone (DHT), stimulate prostate cancer cell growth. By reducing these hormones or blocking their effects, tumor growth can slow significantly, and in some cases, the disease may enter remission.
Approved hormone treatments
There are several approved hormone-based therapies for prostate cancer:
- GnRH agonists, such as leuprolide (Eligard, Lupron) and goserelin (Zoladex), decrease testosterone production by the testicles.
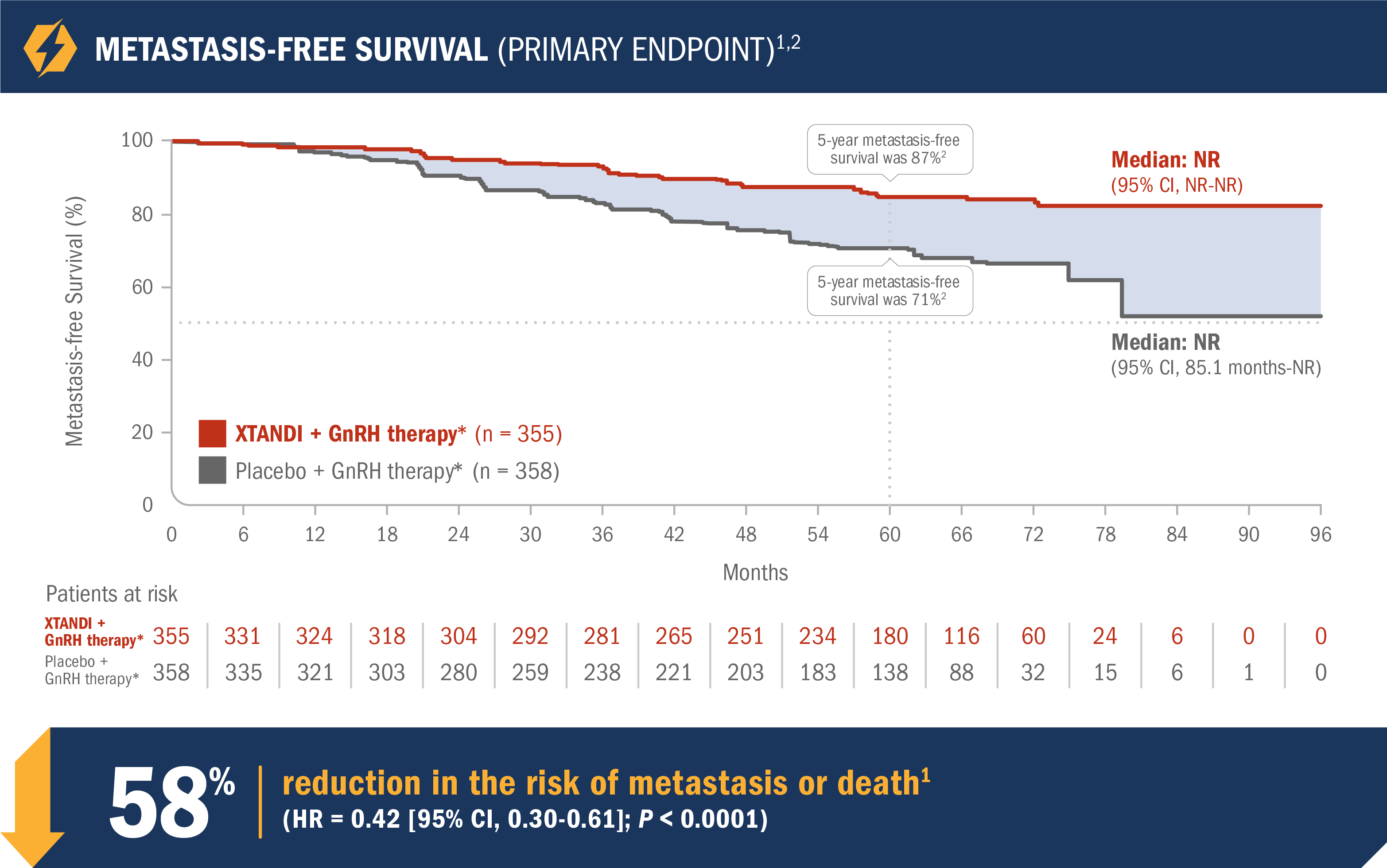
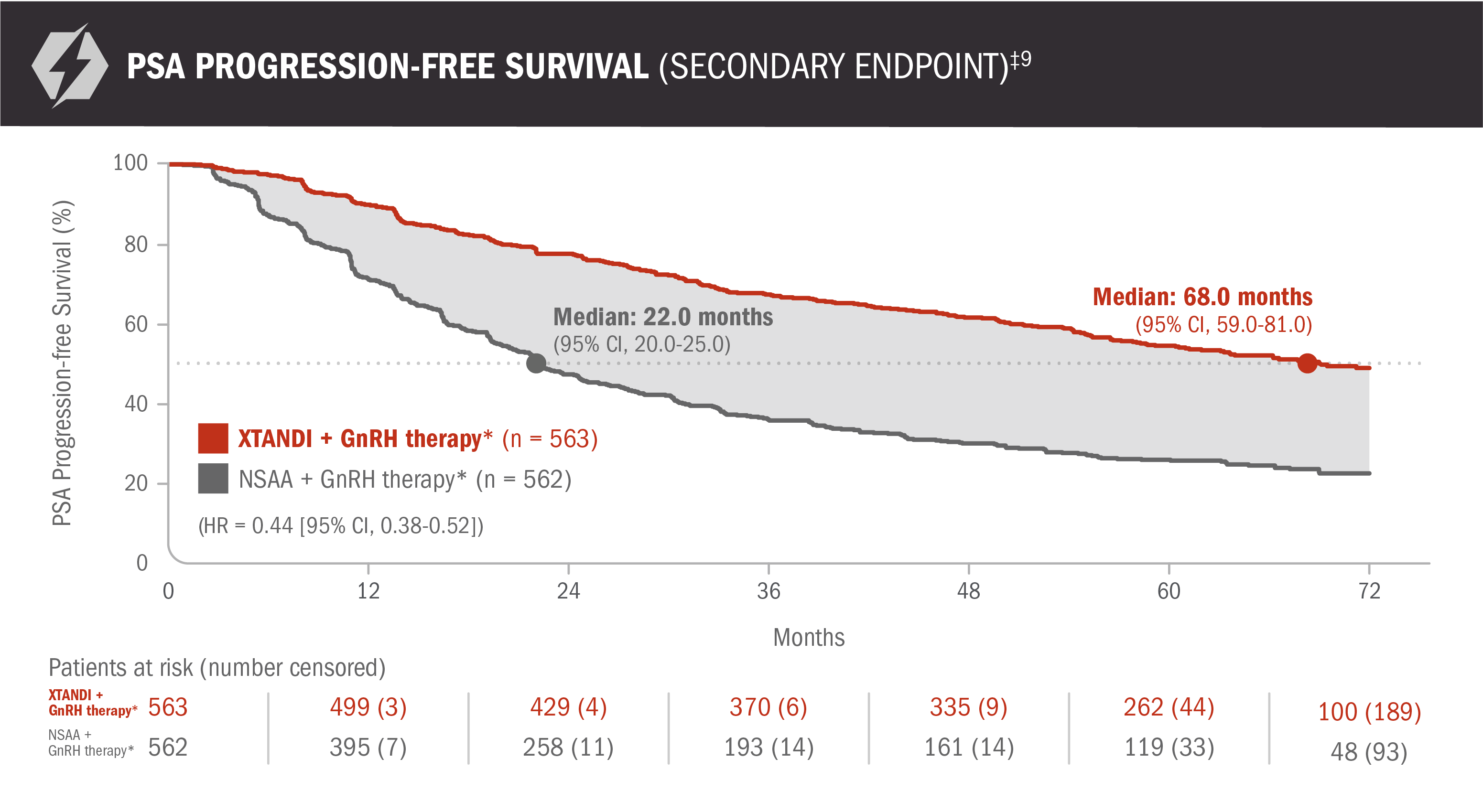
- Anti-androgens, including nilutamide (Nilandron) and enzalutamide (Xtandi), are commonly combined with GnRH agonists to block testosterone from binding to cancer cells.
- Degarelix (Firmagon), a GnRH antagonist, stops signals from the brain to the testes, halting androgen production.
- Orchiectomy, the surgical removal of the testicles, permanently eliminates the primary source of male hormone production.
- Abiraterone (Zytiga), an LHRH antagonist, inhibits the CYP17 enzyme to block androgen production throughout the body.
Treatment goals
The primary aim of hormone therapy is remission, meaning signs and symptoms of prostate cancer diminish or disappear. Although remission does not equal a cure, many people live for years without detectable progression.
Hormone therapy may also be used after initial treatment to reduce the likelihood of recurrence in those at elevated risk.
How treatments are given
- GnRH agonists are administered via injection or implanted beneath the skin.
- Anti-androgens are taken orally, typically once daily.
- Degarelix is delivered by injection.
- Zytiga is taken by mouth once daily alongside prednisone.
The chemotherapy drug docetaxel (Taxotere) is sometimes combined with hormone therapy to enhance effectiveness in certain cases.
Orchiectomy is usually performed as an outpatient procedure, allowing you to return home the same day.
Candidates for hormone therapies
Most individuals with advanced prostate cancer are eligible for hormone therapy, especially when the cancer has spread beyond the prostate gland and surgical removal of the tumor is no longer feasible.
Before starting therapy, doctors often perform liver function testing and blood work to confirm your body can safely metabolize the medications.
Enzalutamide (Xtandi) is approved for people whose prostate cancer has metastasized and no longer responds to treatments aimed at lowering testosterone. However, some cancers eventually become hormone-resistant or castration-resistant, continuing to grow despite low testosterone levels.
When this occurs, monotherapy is generally insufficient. Additional medications that block androgen receptors or alternative systemic treatments may be introduced. Patients and families often begin asking about Life expectancy after Xtandi fails, but outcomes vary widely depending on overall health, cancer burden, and response to subsequent therapies.
In addition to medication adjustments, supportive strategies such as maintaining a balanced diet, engaging in regular physical activity, and reviewing Foods to avoid when taking Xtandi can help optimize overall well-being during treatment.
Common side effects
- hot flashes
- osteoporosis due to decreased testosterone and calcium loss
- weight gain
- reduced muscle mass
- erectile dysfunction
- decreased libido
What is life like after hormone therapy for prostate cancer?
According to the National Cancer Institute, many emotional and sexual side effects associated with low testosterone improve once hormone therapy is discontinued.
Medications such as bisphosphonates may be prescribed to help prevent or reverse bone loss. Weight-bearing exercise and resistance training can also counteract fatigue, muscle loss, and insulin resistance, improving quality of life even in advanced stages.
Nonhormone therapies for advanced prostate cancer
If hormone therapy is no longer effective or the cancer progresses rapidly, doctors may recommend nonhormone treatments. These therapies are often considered when evaluating Life expectancy after Xtandi fails, as they can extend survival and reduce symptoms.
Approved nonhormone treatments
- Chemotherapy, including docetaxel (Taxotere), cabazitaxel (Jevtana), and mitoxantrone (Novantrone), often combined with prednisone.
- Radiation therapy, which uses high-energy beams or radioactive seeds to destroy cancer cells. Lutetium-177 vipivotide tetraxetan PSMA therapy (Pluvicto) is a newer theranostic medicine for advanced metastatic prostate cancer. It targets prostate-specific membrane antigen (PSMA) on cancer cells.
- Immunotherapy, such as sipuleucel-T (Provenge), which stimulates the immune system to attack cancer cells.
- Radium Ra 223 (Xofigo), a radioactive injection used for prostate cancer that has spread to bone.
Treatment goals
The goal of chemotherapy, radiation, immunotherapy, and targeted radiopharmaceuticals is typically to slow disease progression, relieve symptoms, and prolong survival.
While these treatments are unlikely to cure metastatic prostate cancer, they can meaningfully extend life expectancy and maintain quality of life for many individuals.
Candidates for nonhormone therapy
- PSA levels rise rapidly despite hormone therapy.
- The cancer spreads quickly to distant organs.
- Symptoms worsen, such as bone pain or fatigue.
- Hormone-resistant disease develops.
- The cancer has metastasized to bone.
How treatments are given
Chemotherapy is delivered in cycles lasting several weeks, often followed by rest periods. Multiple cycles may be required. If one chemotherapy regimen stops working, another may be considered.
Sipuleucel-T (Provenge) is administered through three intravenous infusions spaced about two weeks apart.
Radium Ra 223 is given by injection.
Common side effects of chemotherapy
- hair loss
- nausea and vomiting
- diarrhea
- fatigue
- loss of appetite
- neutropenia and increased infection risk
- memory changes
- numbness or tingling in extremities
- easy bruising
- mouth sores
Common side effects of radiation therapy
Radiation may lower red blood cell counts, leading to anemia and symptoms such as fatigue, dizziness, and headache. It can also contribute to urinary incontinence and erectile dysfunction.
What happens if you do not treat prostate cancer
Without treatment, most prostate cancers eventually spread beyond the prostate to surrounding tissues and distant organs. However, progression rates differ significantly between individuals.
Some people with low- or intermediate-risk disease may choose active surveillance. In select cases, the cancer may remain stable for years without causing symptoms.
Once the cancer extends beyond the prostate or produces symptoms, active treatment is generally advised.
Takeaway
Hormone therapy and surgery are commonly the first steps in managing advanced prostate cancer.
Prostate cancer is often controlled longest with anti-androgen therapies. When resistance develops — including progression despite enzalutamide (Xtandi) — doctors may turn to chemotherapy, immunotherapy, or radiopharmaceutical treatments such as Radium 223 or Lutetium-177 vipivotide tetraxetan PSMA therapy.
Although metastatic prostate cancer is rarely curable, many treatments can slow its growth, ease symptoms, and extend survival. Concerns about Life expectancy after Xtandi fails are understandable, but many individuals live for years with appropriate follow-up therapy and supportive care.
Deciding among these options can feel overwhelming. Partnering closely with your oncologist and care team ensures you receive personalized guidance, helping you make informed choices aligned with your goals and values.




















Leave a Reply
You must be logged in to post a comment.