
Key takeaways
- You may need to change prostate cancer treatments if the disease progresses, side effects become difficult to tolerate, or current medications negatively interact with other drugs.
- Indicators that your present prostate cancer therapy may no longer be effective include changes on radiographic imaging, worsening PSA blood test patterns, or new and intensifying symptoms such as bone pain or fatigue.
- Clear, open communication with your oncologist is essential when considering a treatment change, so you can review your goals, potential side effects of alternative therapies, and overall quality of life.
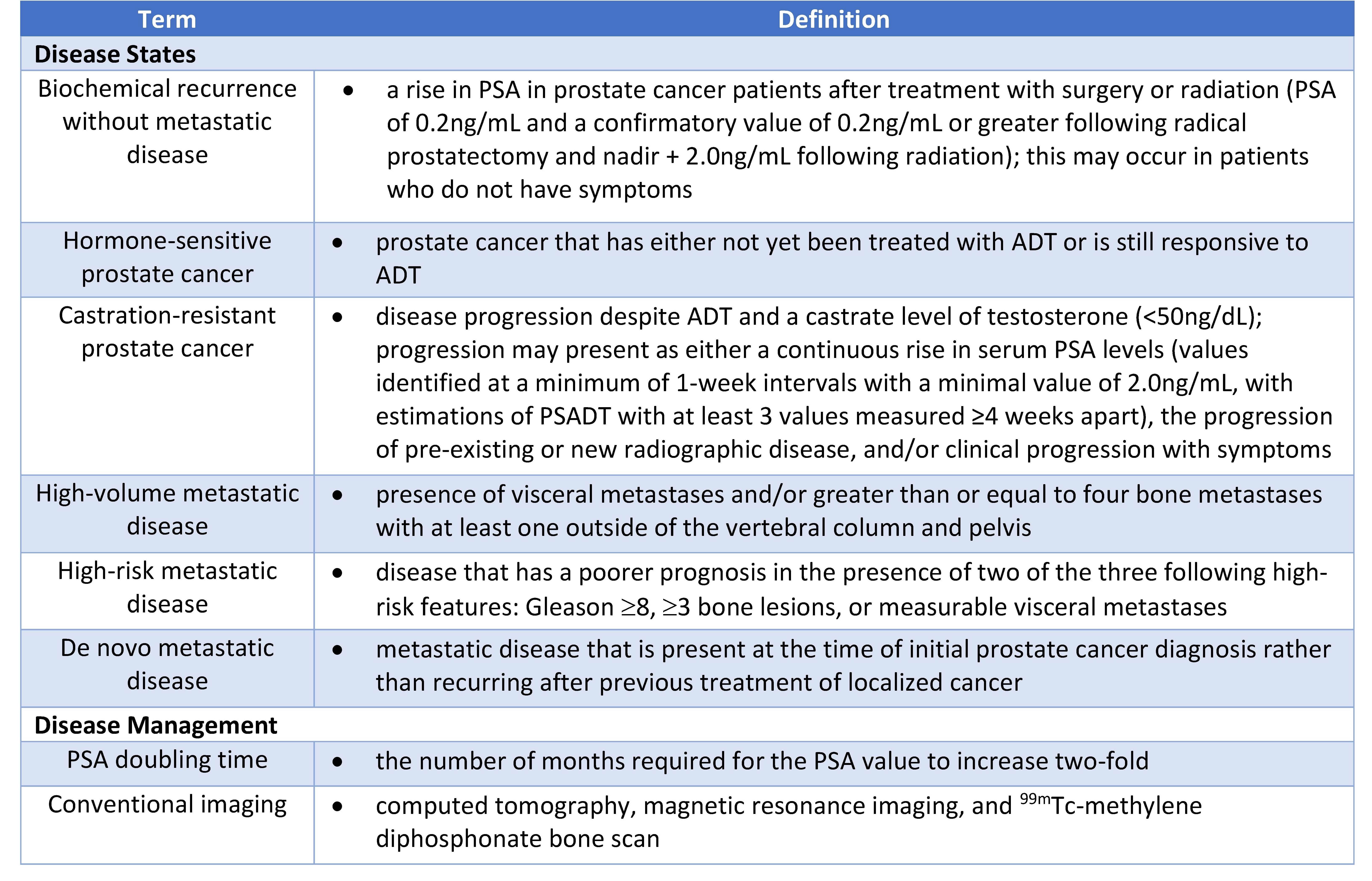
Switching therapies in prostate cancer care is relatively common and can happen for a variety of reasons. In discussions about PSA doubling time guidelines and disease monitoring, many patients learn that treatment adjustments are sometimes part of long-term management. Options for advanced prostate cancer include injections, oral medications, intravenous chemotherapy, and radiopharmaceutical agents delivered through an IV.
What happens when you change your prostate cancer treatment?
The most frequent reason for changing prostate cancer therapy is cancer progression, meaning the cancer is spreading or increasing in size despite ongoing treatment. In clinical terms, this is referred to as “progression of the cancer.”
Oncologists often describe treatments as “first-line” or “second-line” therapy, depending on how many prior regimens a patient has received. When a transition is made from one line of therapy to another because of progression, the current medication is typically discontinued and the new therapy is initiated, often without a significant delay.
Another common reason for modifying prostate cancer treatment is the development of intolerable side effects. Every medication used in prostate cancer management carries potential adverse effects, although not every patient will experience them.
One frequently prescribed medication is leuprolide (Lupron) injection. The prescribing information lists numerous possible side effects, including suicidal ideation. While most individuals do not develop these thoughts, anyone who does should promptly discuss alternative treatment options with their oncology team.
If a treatment change is being considered due to bothersome but non-life-threatening side effects, your clinician may first attempt lowering the dose or adjusting how often the medication is given before stopping it completely. This approach is commonly used for symptoms such as:
- intolerable fatigue
- hot flashes
- diarrhea
- joint aches
- weakness
However, if the adverse effect is life-threatening (for example, suicidal ideation), the safest course is usually to stop the medication immediately rather than attempt a dose reduction.
Treatment changes may also occur because of “drug-drug interactions” or DDI. This situation arises when two medications interact in a way that alters how one is metabolized, potentially leading to increased side effects or reduced effectiveness.
In these circumstances, there may be another medication within the same class that works through a similar mechanism but does not interact with your other prescriptions.
For instance, in prostate cancer patients with a history of blood clots who are taking the blood thinner apixaban, a potential drug–drug interaction exists with apalutamide, an oral medication commonly used in prostate cancer treatment.
Using these two drugs together can decrease the effectiveness of the blood thinner, increasing the risk of clot formation.
An oncologist may collaborate with a pharmacist to determine which agents within the classes of Apixiban or Apalutamide would be reasonable alternatives to avoid a DDI.
When a switch is required, it typically involves changing just one medication. The transition may happen immediately or after a brief “wash out period” to prevent supratherapeutic (higher-than-safe) drug levels, especially if the prior interaction caused elevated concentrations in the bloodstream.
What signs suggest treatment is no longer working?
The clearest signs that prostate cancer therapy is failing include an increased cancer burden on radiographic images, the appearance of new lesions, or worsening serum tumor markers. In prostate cancer, commonly used radiographic imaging modalities include PSMA PET scan, CT scan, and bone scan to identify cancer location and assess its extent.
MRI may also be used, though it is less common in this context. For individuals with advanced prostate cancer, imaging is performed at scheduled intervals—often months apart—to evaluate response to therapy. Each new scan is compared with prior imaging in what is known as a “restaging scan.”
Unlike some other cancers, prostate cancer often has a reliable blood-based tumor marker: prostate-specific antigen (PSA). This protein is produced by prostate cells, including malignant ones.
PSA levels are generally checked every 3 to 6 months. Rather than focusing solely on the absolute PSA value, clinicians pay close attention to the overall trend. Rising PSA levels over time may indicate reduced treatment effectiveness. Understanding PSA doubling time guidelines can provide additional insight into how aggressive the cancer may be becoming and whether therapy adjustments are needed.
The doubling time of a PSA (PSADT) has been shown to help predict when prostate cancer is becoming more aggressive and more likely to spread. Many patients and clinicians use tools such as a PSA velocity calculator to better understand PSA kinetics, which can complement established PSA doubling time guidelines in ongoing monitoring.
In addition to imaging and lab results, new or worsening symptoms may signal that a medication is no longer effective. Examples include new bone pain, increasing fatigue, reduced appetite, or worsening urinary issues.
If these symptoms are caused by cancer progression, they generally persist or intensify until treatment is modified.
What makes oral medicines like Orgovyx different from injectable hormone therapy?
Historically, hormonal blockade therapy for prostate cancer involved surgical castration of the testicles. Over time, medical alternatives were developed that manipulate GnRH (gonadotropin-releasing hormone) agonists or antagonists to suppress testosterone production.
A GnRH agonist initially causes a temporary surge in testosterone before ultimately lowering levels. In contrast, a GnRH antagonist produces a rapid decline in testosterone without that initial surge.
An oral option, relugolix (Orgovyx), is a GnRH antagonist. It shares many side effects with injectable GnRH therapies but avoids injection-site reactions such as pain or swelling.
Oral therapies like relugolix have side effects comparable to injectable GnRH treatments, including:
- fatigue
- hot flashes
- sexual dysfunction
- bone loss
- heart problems
The main disadvantage of an oral GnRH antagonist such as relugolix is the need for strict daily adherence. Missing doses could affect testosterone suppression. The advantage is the absence of injection-related side effects.
Other oral agents target the androgen receptor or androgen synthesis. These medications have distinct side effect profiles and cannot replace injectable GnRH agonists or antagonists, as they reduce prostate cancer activity through different biological mechanisms.
How do I bring up switching treatment with my doctors?
If your prostate cancer therapy is controlling the disease but significantly diminishing your quality of life, deciding what to do next can feel overwhelming.
In advanced stages, especially when cancer has spread to distant sites, treatment may be palliative. In this setting, maintaining quality of life (QoL) becomes a primary focus alongside cancer control.
Hormonal blockade and other systemic therapies for prostate cancer often produce side effects such as:
- fatigue
- hot flashes
- sexual dysfunction
- joint discomfort
- lack of concentration/motivation
These effects can lead some individuals to question whether continuing treatment to extend survival aligns with their personal priorities. This is a valid and deeply personal consideration.
Having an honest discussion with your oncologist about your goals, expectations, and understanding of PSA trends—including how PSA doubling time guidelines apply to your case—can help clarify the best path forward. Expressing concerns about side effects and how they impact daily living is a critical component of a strong doctor–patient relationship.
Early conversations about treatment objectives can make future decisions less stressful and more aligned with your values.
What questions should I ask my doctor about switching treatments?
If a therapy change is proposed, your first step should be understanding the reason. Treatment adjustments may be due to:
- progression of the cancer
- lab abnormalities
- intolerable side effects
- medicine-to-medicine interactions
It is appropriate to ask whether the new therapy has side effects similar to or different from your current medication.
You may also want to discuss how likely the new treatment is to meet its intended goal, how long it is expected to continue, how it will be administered, and whether it should begin immediately or after a short washout period from the prior drug.
Takeaway
Changing prostate cancer treatments is a common aspect of care and usually occurs because of cancer progression, unacceptable side effects, or medication interactions.
Ongoing monitoring with imaging, PSA trends, symptom assessment, and reference to PSA doubling time guidelines helps determine when a transition is appropriate. Maintaining open communication with your oncologist about treatment goals, potential side effects, and quality of life remains essential when considering any change in therapy.





















Leave a Reply
You must be logged in to post a comment.