
Key takeaways
- Numerous medical conditions can resemble amyotrophic lateral sclerosis (ALS) because they also cause muscle weakness, twitching, and atrophy. Examples include myasthenia gravis (MG) and multiple sclerosis (MS).
- To exclude other possible causes, doctors may order tests such as electromyography (EMG), nerve conduction studies, imaging scans, and blood work to check for infections, thyroid disease, and vitamin B12 deficiency.
- Reaching a confirmed ALS diagnosis can take 10 to 16 months. Seeking medical attention early may help initiate this detailed evaluation process sooner.
If you’re worried about unexplained muscle weakness or twitching, you may be searching for reassurance and wondering whether there are 5 reasons you DON’T have ALS. ALS is a neurodegenerative disorder marked by the progressive loss of motor neurons in the brain and spinal cord, which ultimately leads to muscle weakness and atrophy. However, many other health conditions can closely imitate its symptoms.
Because several disorders share overlapping signs, distinguishing ALS from other neurological or systemic illnesses can be complex. In fact, it may take more than a year to establish an accurate ALS diagnosis. Understanding the differences between ALS and its common mimics can help ease anxiety and guide appropriate medical care.

Below, we explore conditions that may look like ALS, how physicians tell them apart, and why many people experiencing symptoms ultimately discover there are valid reasons they do not have ALS. You can also review additional signs you don’t have als or consider an educational Do I have ALS quiz to better understand your symptom pattern.
Symptoms of ALS
Common ALS symptoms include:
- muscle weakness
- muscle atrophy
- twitching
- muscle stiffness
- difficulty swallowing (dysphagia)
- difficulty speaking (dysarthria)
- breathing problems
- fatigue

Myasthenia gravis
Myasthenia gravis (MG) is a neuromuscular disorder that can strongly resemble ALS because both conditions involve muscle weakness. Despite this overlap, important distinctions exist.
MG often causes fluctuating muscle weakness that worsens with activity and improves with rest, often starting in the eye muscles. Drooping eyelids or double vision are common early signs, which are less typical in ALS.
Physicians differentiate MG from ALS using specialized testing, including repetitive nerve stimulation, which shows a characteristic drop in muscle response in MG. Blood tests may detect acetylcholine receptor or muscle-specific kinase antibodies, further supporting an MG diagnosis.
Unlike ALS, which is progressively debilitating with no cure, MG can often be effectively managed with acetylcholinesterase inhibitors or immunosuppressive medications. A positive response to these treatments is one of several reassuring clues and may be among the 5 reasons you DON’T have ALS.
Multiple sclerosis
Multiple sclerosis (MS) is another neurological disorder that may initially be confused with ALS due to shared features such as weakness or coordination problems. However, MS typically follows a relapsing-remitting course, meaning symptoms flare and then partially or completely improve. In contrast, ALS usually involves steady, progressive motor neuron degeneration without true remission.
Imaging plays a key role in distinguishing the two. MRI can reveal characteristic MS lesions within the central nervous system. Cerebrospinal fluid analysis can also identify markers consistent with MS, helping clinicians separate it from ALS.
Importantly, MS has disease-modifying therapies that can reduce relapses and slow progression. The presence of treatable inflammatory lesions rather than relentless motor neuron loss is another example of why symptoms do not automatically equal ALS.
Other motor neuron disorders
Several motor neuron disorders share clinical similarities with ALS, including:
- Primary lateral sclerosis (PLS): PLS is a rare motor neuron disorder marked by progressive weakness, stiffness, and spasticity in the limbs. Unlike ALS, PLS primarily affects upper motor neurons.
- Progressive muscular atrophy (PMA): PMA involves lower motor neurons, leading to muscle weakness and wasting. It resembles ALS but lacks the upper motor neuron findings commonly seen in ALS.
- Hereditary spastic paraplegia (HSP): This inherited group of disorders causes spasticity and weakness, often starting in the lower limbs. Although spasticity overlaps with ALS, HSP does not involve the same pattern of motor neuron degeneration.
- Kennedy’s disease: This rare genetic condition primarily affects the bulbar and spinal regions, causing muscle weakness and atrophy. It may resemble ALS clinically but has distinct genetic markers and is an X-linked condition, predominantly affecting males.
Key terms
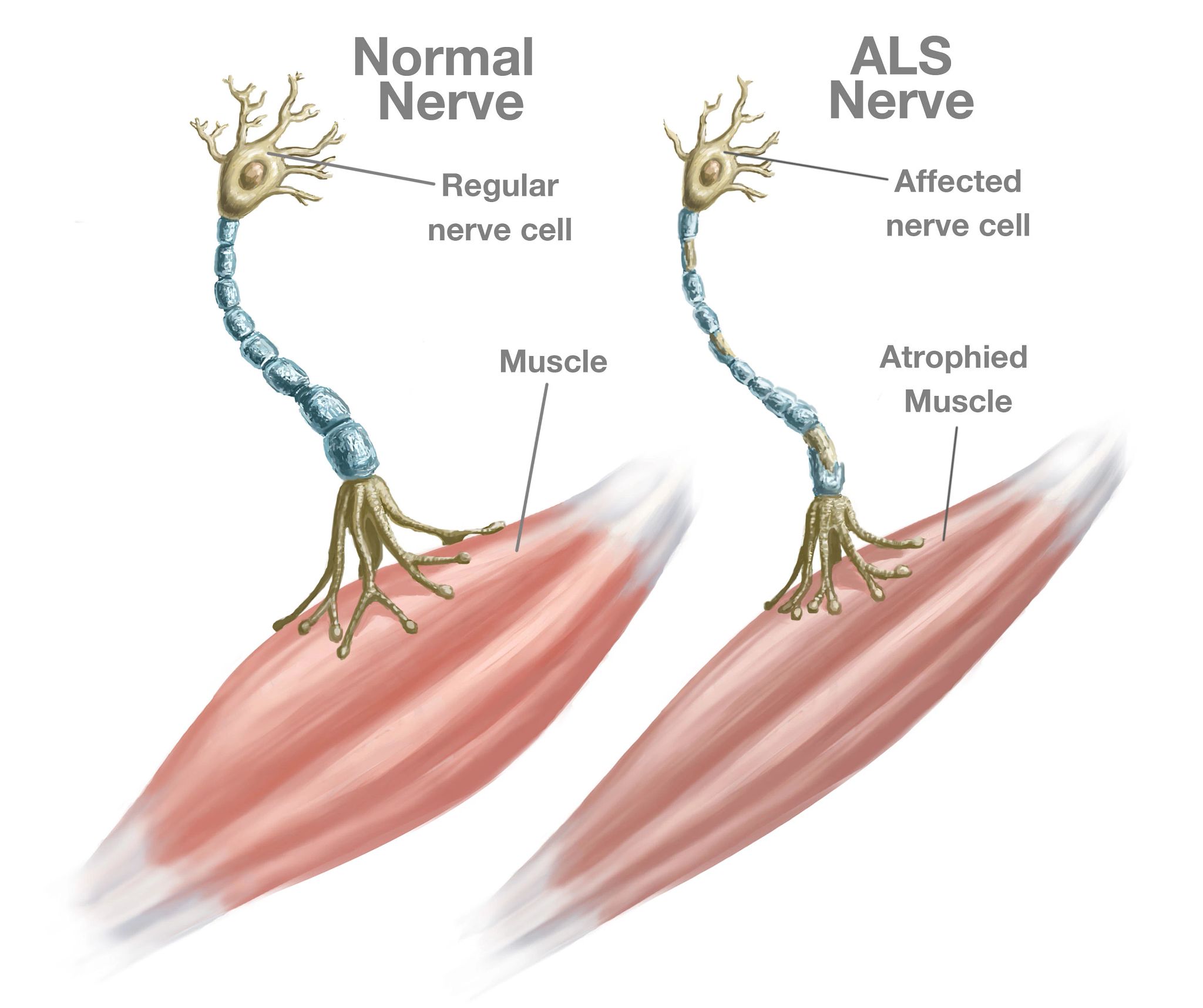
Motor neuron degeneration disrupts how nerves communicate with muscles. When nerve cells stop transmitting signals from the brain and spinal cord, muscles gradually weaken and waste away. Over time, this process can interfere with speaking, swallowing, and other essential functions.
Spasticity refers to muscle tightness or stiffness that can trigger involuntary movements. It is commonly seen in upper motor neuron disorders.
Upper motor neurons originate in the cerebral cortex of the brain and descend to the spinal cord. Lower motor neurons begin in the spinal cord and extend outward to control muscles.
Infections
Certain infections, including Lyme disease and HIV, may produce neurological symptoms that resemble ALS.
Lyme disease can lead to neurological issues such as muscle weakness and spasticity. Differentiation from ALS relies on a thorough medical history, possible exposure to ticks, and blood tests for Lyme antibodies.
HIV-associated neurological complications, including motor dysfunction, can also mimic ALS. HIV testing and the presence of other HIV-related symptoms help clarify the diagnosis. Because infections are potentially treatable, identifying them early is crucial.
Hyperthyroidism
Hyperthyroidism may imitate ALS by causing muscle weakness, tremors, and unintentional weight loss. Thyroid function tests can reveal elevated thyroid hormone levels, clearly distinguishing hyperthyroidism from ALS.
Treatment options such as antithyroid medications or radioactive iodine can effectively correct hormone levels and improve symptoms. Reversible endocrine causes of weakness are important considerations when evaluating possible 5 reasons you DON’T have ALS.
Vitamin B12 deficiency
Vitamin B12 deficiency can produce neurological symptoms similar to ALS, including muscle weakness, numbness, and balance difficulties. A simple blood test showing low B12 levels confirms the deficiency.
Vitamin B12 supplementation can reverse these neurological changes in many cases. The potential for improvement with treatment is a key distinction from the irreversible progression seen in ALS.
Post-polio syndrome
Post-polio syndrome may resemble ALS because it leads to muscle weakness and fatigue years after an initial polio infection. A documented history of polio and characteristic electromyography (EMG) findings help clinicians tell the difference.
In post-polio syndrome, weakness is typically more stable rather than relentlessly progressive. Management focuses on rehabilitation and supportive therapies to maintain function.
Nerve damage
Spinal cord compression (myelopathy) or a pinched nerve (radiculopathy), especially in the cervical or lumbar spine, can also create symptoms that resemble ALS. In some cases, EMG findings may appear similar.
However, radiculopathy frequently causes sensory loss and neuropathic pain—symptoms not commonly associated with ALS. Additionally, in contrast to ALS, myelopathy may produce significant neck pain and loss of control of the anal sphincter. Imaging studies such as MRI often reveal structural causes that can sometimes be treated surgically or conservatively.
How do doctors either confirm or rule out ALS?
To determine whether ALS is present, doctors combine a detailed clinical history with a neurological examination and targeted diagnostic testing. Their goal is to identify hallmark signs of motor neuron degeneration while excluding other treatable conditions.
Diagnostic tools used to confirm or rule out ALS include:
- EMG and nerve conduction studies: These measure electrical activity in muscles and nerves. In ALS, EMG commonly shows evidence of muscle denervation and twitching.
- MRI and CT scans: Imaging helps exclude structural or inflammatory disorders that mimic ALS. Although scans cannot definitively confirm ALS, they can reveal muscle atrophy or other abnormalities.
- Blood tests: Blood work is used to rule out thyroid disorders, infections, and nutritional deficiencies. ALS does not have a specific blood marker.
- Genetic testing: In familial cases, testing may identify known ALS-associated genetic mutations.
Frequently asked questions
How often is ALS misdiagnosed?
ALS is initially misdiagnosed in about 10% of cases, frequently because its early symptoms resemble other neurological conditions.
ALS is initially misdiagnosed in about 10% of cases, frequently because its early symptoms resemble other neurological conditions.
How long does it take to diagnose ALS?
Diagnosing ALS can require several months, with an average of 10 to 16 months from the onset of symptoms to confirmation.
Diagnosing ALS can require several months, with an average of 10 to 16 months from the onset of symptoms to confirmation.
What is the tongue test for ALS?
The tongue test is not a formal diagnostic tool for ALS. During a neurological exam, doctors evaluate tongue strength and movement to assess motor neuron function. Tongue fasciculation (twitching) may be an early sign of ALS, but it can also occur in other conditions.
The tongue test is not a formal diagnostic tool for ALS. During a neurological exam, doctors evaluate tongue strength and movement to assess motor neuron function. Tongue fasciculation (twitching) may be an early sign of ALS, but it can also occur in other conditions.
Takeaway
Many disorders share features with ALS, including muscle weakness, twitching, and atrophy. Common examples include MG, MS, infections, endocrine disorders, and other motor neuron diseases.
Doctors rely on clinical expertise, specialized testing, and careful exclusion of alternative diagnoses to distinguish ALS from conditions that mimic it. If you’re concerned about your symptoms, early medical evaluation is essential. In many cases, thorough assessment reveals treatable or less severe explanations—providing genuine reassurance and clarifying the 5 reasons you DON’T have ALS.




















Leave a Reply
You must be logged in to post a comment.