
During the first four weeks of pregnancy, hCG concentrations generally double roughly every 48 to 72 hours. If there’s concern for miscarriage, hCG levels are more likely to fail to double or to fall.
Human chorionic gonadotropin (hCG) is a hormone produced during pregnancy that helps sustain fetal development.
Clinicians check hCG in blood and urine to verify pregnancy. They also use serial hcg blood measurements to assist in evaluating the possibility of an ectopic pregnancy or a miscarriage.
Pregnancy, an ectopic implantation, and pregnancy loss are never diagnosed from a single hCG measurement alone, but knowing typical hCG behavior is useful in these situations.
hCG behavior in early pregnancy
If you suspect you’re pregnant, your provider will measure your hCG by drawing blood from a vein.
No detectable hCG in a blood test doesn’t automatically rule out pregnancy — it may simply be too early for levels to have risen yet.
Values above 5 milli-international units per milliliter (mIU/mL) generally indicate pregnancy. That initial test serves as a baseline and can span from very low amounts (for example, around 20 mIU/mL or less) to much higher numbers (for example, near 2,500 mIU/mL).
The baseline matters because of “doubling time.” In a viable pregnancy during those first four weeks, hCG typically doubles every two to three days. After about six weeks, the doubling interval lengthens to roughly 96 hours.
So if your baseline exceeds 5 mIU/mL, your clinician may repeat the test a few days later to verify an expected doubling.
Absent specific risk factors, one or two measurements may be sufficient to confirm pregnancy. Often, clinicians will then suggest an ultrasound between 8 and 12 weeks as part of routine first-trimester care.
hCG patterns in miscarriage
If there’s a risk of miscarriage or ectopic pregnancy, a failure of hCG to double — or a decline — is more likely. Your clinician may ask you to return 48 to 72 hours after the baseline draw to see whether levels have appropriately increased.
When hCG doesn’t approximately double in that time frame, clinicians may worry the pregnancy is at risk. Medically, this may be labeled a possible “nonviable pregnancy.”
If hCG is falling or rising only slowly, additional testing is usually ordered. This can include measuring progesterone and performing a transvaginal ultrasound to search for a gestational sac in the uterus. Symptoms such as bleeding or cramping are also considered.
In a miscarriage, hCG commonly declines compared with earlier values. For instance, a baseline of 120 mIU/mL that falls to 80 mIU/mL two days later suggests the embryo is no longer developing and hormonally unsupported.
Similarly, very slow rises — for example, from 120 mIU/mL to 130 mIU/mL over two days — may indicate a nonviable intrauterine pregnancy that could miscarry soon.
Slow-rising hCG can also signal a non-uterine implantation, typically in the fallopian tube. Because an ectopic pregnancy can be emergent, timely identification is crucial.
However, it’s possible for hCG to double even with an ectopic pregnancy. That is why hCG trends alone don’t provide absolute certainty about the pregnancy’s status.
Do low hCG levels always mean miscarriage?
A low initial hCG isn’t necessarily problematic by itself. Normal hCG ranges at different early-pregnancy stages are wide.
For example, a day after a missed period, hCG might be only 10–15 mIU/mL, or it could exceed 200 mIU/mL. Pregnancies vary greatly in this regard.
What’s most important is the pattern over time. Different people may start with different baselines and still carry to term.
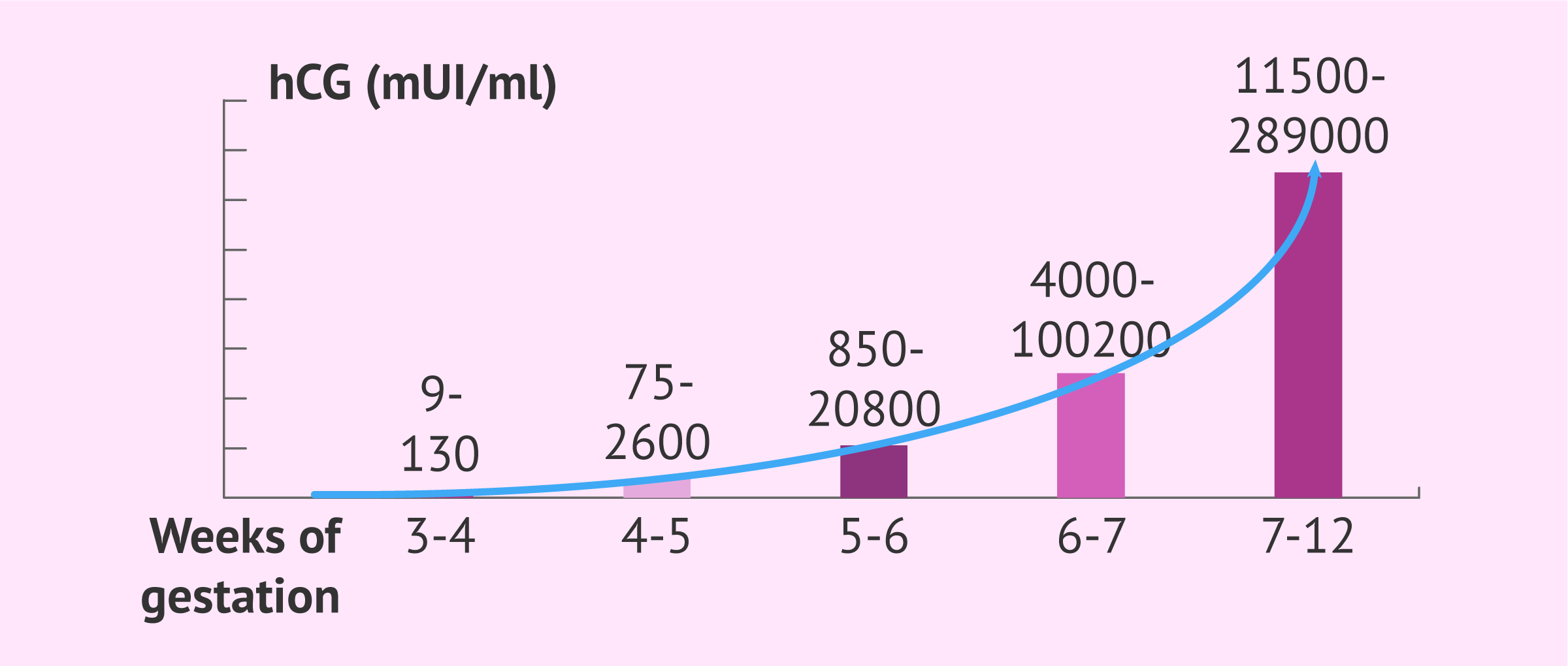
The table below displays common hCG ranges during pregnancy.
| Weeks since last missed period | hCG mIU/mL (or IU/L) |
| 3 weeks | 5 to 50 |
| 4 weeks | 5 to 426 |
| 5 weeks | 19 to 7,340 |
| 6 weeks | 1,080 to 56,500 |
| 7 to 8 weeks | 7,760 to 229,000 |
| 9 to 12 weeks | 25,700 to 288,000 |
| 13 to 16 weeks | 13,300 to 254,000 |
| 17 to 24 weeks | 4,060 to 165,400 |
| 25 to 40 weeks | 3,640 to 117,000 |
Do falling hCG levels always signal miscarriage?
When hCG declines, the prognosis for the pregnancy is generally unfavorable.
Laboratory error is possible, or other conditions — such as ovarian hyperstimulation syndrome (OHSS) after fertility therapy — can alter hormone readings.
Nevertheless, decreasing hCG after a positive result is usually a poor sign and often indicates a nonviable pregnancy, as reported in the journal Fertility and Sterility.
Does a very slow rise always mean miscarriage?
A gradual hCG increase doesn’t definitively mean a miscarriage, but it typically prompts further evaluation.
Clinicians rely on data, often from smaller studies of assisted conceptions, to guide interpretation of hCG trends, according to Fertility and Sterility. While helpful for next steps, hCG numbers aren’t absolute indicators of either miscarriage or a healthy pregnancy.
Doubling times are primarily used to help confirm a pregnancy rather than to diagnose pregnancy loss. Per Obstetrics & Gynecology, a rise of 53% or more over two days corresponds to a viable pregnancy in about 99% of cases.
Keep in mind the initial hCG matters. Those with a baseline under 1,500 mIU/mL have more potential for rapid proportional increases.
Conversely, someone who is farther along and starts with a high hCG (5,000 mIU/mL or more) usually shows slower proportional rises, as noted in Obstetrics & Gynecology.
Multiple gestations (twins, triplets, etc.) and gestational age can influence the rate of hCG rise.
Ectopic pregnancies and miscarriages often produce lower hCG values; a molar pregnancy tends to cause markedly elevated levels.
How clinicians confirm a miscarriage
Doctors use several tests when confirming a miscarriage, including:
- blood tests such as serial hCG and progesterone
- evaluation of symptoms, like pelvic cramping or vaginal bleeding
- transvaginal ultrasound and pelvic examination
- fetal heart assessment (when dates suggest a heartbeat should be visible)
Clinicians will combine multiple data points before making a miscarriage diagnosis. When a pregnancy is extremely early, falling hCG may be the primary indicator that a loss is likely until additional time allows more definitive imaging.
Promptly identifying a miscarriage or ectopic pregnancy is essential. An untreated ectopic can cause fallopian tube rupture or other harm that jeopardizes fertility and can be life-threatening. Retained tissue after a miscarriage increases the risk of bleeding and infection.
For these reasons, if pregnancy loss occurs, clinicians may recommend medications or surgical procedures to reduce complications.
Pregnancy loss can also be emotionally painful. Receiving a diagnosis can help provide closure and begin the process of grieving and healing.
Returning hCG to zero after a miscarriage
After a miscarriage (and after birth), your body stops producing hCG and levels eventually fall to zero mIU/mL.
Clinically, any value below 5 mIU/mL is considered negative, so 1–4 mIU/mL is effectively treated as zero.
The time it takes hCG to reach zero depends on how high levels were when the miscarriage occurred. Very early losses with low hCG usually return to zero within days.
When hCG was in the thousands or tens of thousands at the time of loss, it can take weeks for levels to normalize, according to the American Association for Clinical Chemistry.
Once levels reach zero, menstruation typically resumes and ovulation returns.
Clinicians usually advise waiting until after the first period before attempting to conceive again, as dating a new pregnancy is easier once cycles resume.
After a dilation and curettage (D&C) for miscarriage, providers may suggest waiting two to three cycles before trying again because a D&C can thin the uterine lining; the endometrium generally rebuilds over several months.
Summary
Early pregnancy loss can be physically and emotionally difficult. If you suspect a miscarriage, contact your clinician. They can run tests, including serial hCG measurements, to clarify the situation.
A miscarriage doesn’t mean you can’t have a successful pregnancy in the future — most people do. Support resources are available for those who experience pregnancy loss; ask your clinician for guidance and referrals.























Leave a Reply
You must be logged in to post a comment.