
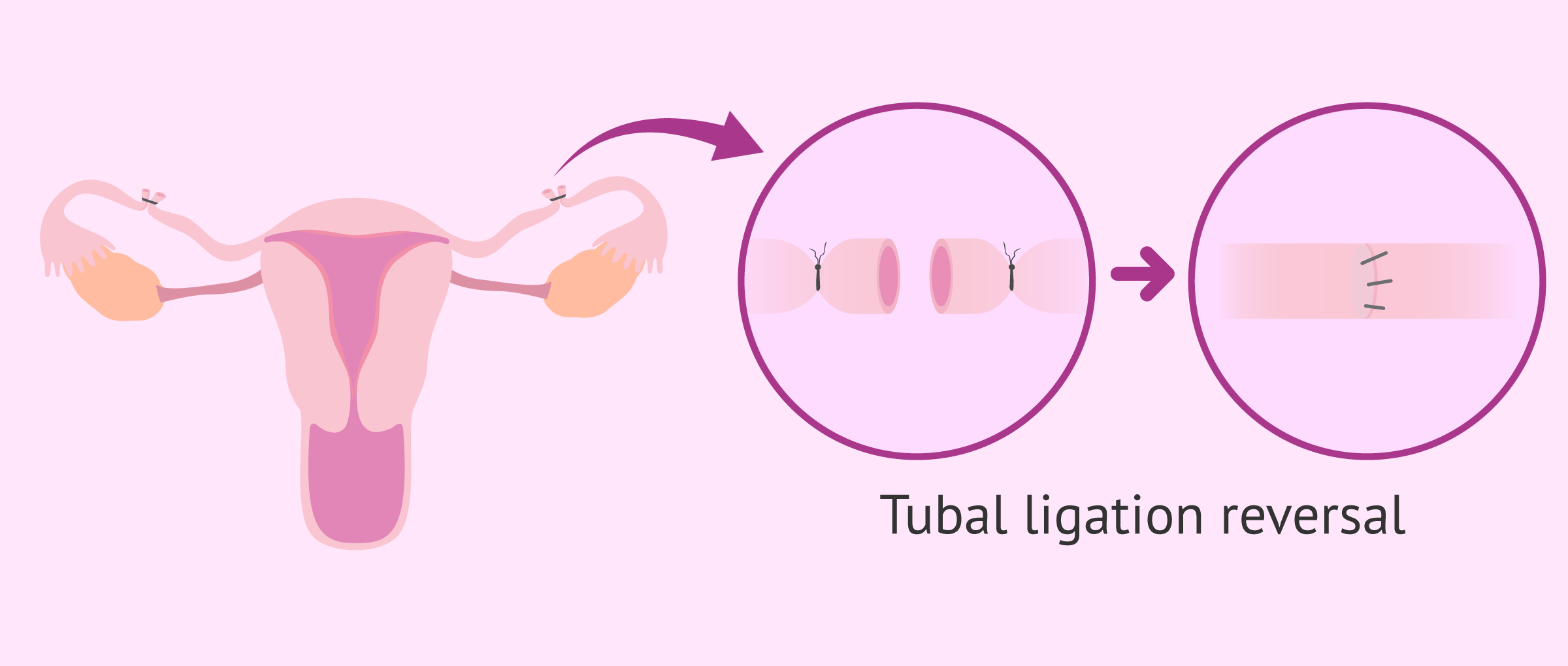
Yes — tubal ligation can sometimes be reversed. Reversal surgery reconnects the separated or obstructed portions of the fallopian tubes, enabling someone who previously had their tubes tied to conceive naturally.
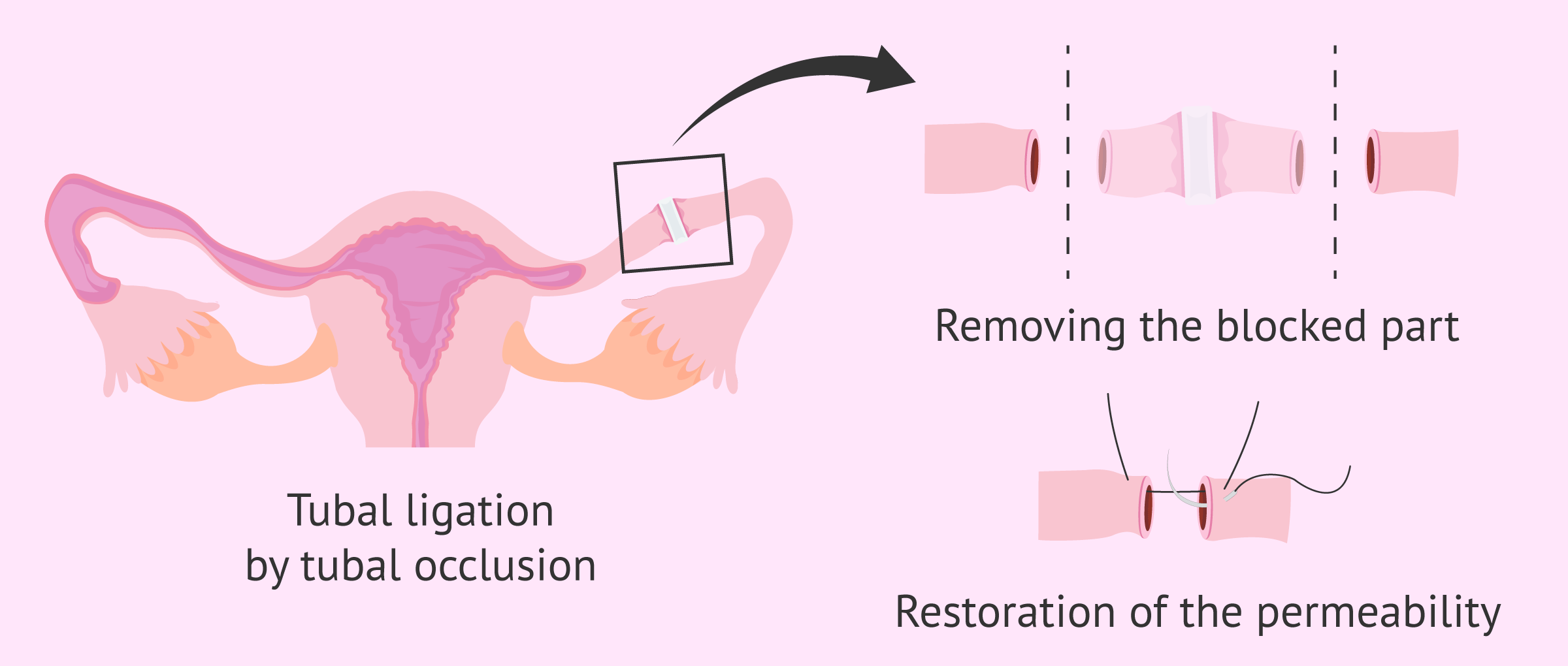
In a tubal ligation (commonly called “having your tubes tied”), the fallopian tubes are cut, sealed, or otherwise blocked. Since fertilization typically occurs within the fallopian tube, tubal ligation prevents pregnancy by stopping sperm and egg from meeting.
Tubal ligation reversal is also referred to as tubal reanastomosis, tubal reversal, or tubal sterilization reversal.
About 1 percent of tubal sterilizations are eventually reversed.
Who is a good candidate?
Several factors influence the likelihood of success for a tubal ligation reversal:
- Type of sterilization: Certain sterilization techniques cannot be successfully reversed.
- Amount of healthy tube remaining: Reversal outcomes are better when a substantial portion of undamaged fallopian tube is present.
- Age: Younger patients tend to have higher success rates with reversal.
- Body mass index: Being overweight or obese may reduce the chances of a successful reversal.
- Other medical conditions: Health issues such as autoimmune disorders can affect fertility; these will be considered when determining if reversal is appropriate.
- Overall fertility: Existing fertility problems in either partner lower the probability of success. Before surgery, physicians commonly evaluate both partners — checking sperm quality, ovarian reserve, and imaging the uterus — to assess the chances of pregnancy.
How much does it cost?
The typical cost for a tubal ligation reversal in the United States is about $8,685. Depending on the region, required preoperative testing, and other variables, total expenses can range from roughly $5,000 up to $21,000. Insurance policies rarely cover this procedure, though many clinics offer financing or payment plans.
What occurs during the operation?
Initially, the surgeon inspects the fallopian tubes using a laparoscopic camera — a tiny camera inserted into the abdomen through a small incision. If enough healthy tube is present and there are no other contraindications, the surgeon proceeds with the reversal.
Most reversals are performed laparoscopically. The surgeon makes several small abdominal incisions (the largest about ½ inch), inserts the camera and instruments, and operates while viewing the procedure on a monitor. The operation typically lasts two to three hours and is done under general anesthesia.
Damaged portions of the tubes and any sterilization devices (such as clips or rings) are removed. The surgeon then uses very fine sutures to join the healthy ends of the fallopian tubes. After reattachment, dye is injected into each tube; if the dye does not leak, it indicates the tube has been successfully rejoined.
In some cases, a minilaparotomy is used. The surgeon makes a slightly larger incision (about 2 inches), exteriorizes the tube ends through the incision, trims damaged segments, and reconnects the healthy portions while the tubes are outside the body.
What is the recovery and postoperative timeline?
If the procedure and immediate recovery go smoothly, most people can return home about three hours after surgery. Recovery after a laparoscopic reversal usually takes around one week, whereas recovery after a minilaparotomy is closer to two weeks.
During recovery you can expect some pain and tenderness near the incision sites. Your doctor may prescribe pain medication or recommend over-the-counter options. For a few days you may experience shoulder discomfort from the gas used to expand the abdominal cavity during laparoscopy; lying down often eases this pain.
Avoid bathing for 48 hours after surgery; gently pat the incision site rather than rubbing it. Refrain from heavy lifting and sexual intercourse for the period your surgeon advises. Apart from these precautions, there are generally no strict dietary or activity limitations.
You should have a follow-up appointment with your surgeon about one week after the operation.
What are the chances of pregnancy?
Overall, about 50 to 80 percent of people who undergo tubal ligation reversal achieve a successful pregnancy.
Variables that influence success include:
- Partner’s sperm quality: Pregnancy odds improve when both partners have no fertility issues.
- Length of healthy tube remaining: Less damage to the fallopian tubes at the time of the original sterilization increases chances of conception.
- Pelvic adhesions: Scar tissue from prior pelvic surgeries can reduce the likelihood of pregnancy.
- Type of sterilization: Those whose tubes were sterilized with rings or clips generally have higher pregnancy rates after reversal.
- Age: Success is greatest in people under 35 and declines with age. Women younger than 35 have about a 70 to 80 percent pregnancy rate, whereas rates fall to roughly 30 to 40 percent for those over 40.
What complications can occur?
As with any operation, tubal reversal carries risks related to anesthesia, bleeding, or infection; these are uncommon. Your surgeon will discuss these risks before the procedure.
Reversal also raises the risk of an ectopic pregnancy, where a fertilized egg implants outside the uterus — most commonly in a fallopian tube. While ectopic pregnancies account for up to 2 percent of pregnancies overall, the rate after tubal reversal is higher, estimated at 3 to 8 percent.
An ectopic pregnancy is potentially life-threatening without treatment due to risk of severe bleeding. It cannot progress to a normal intrauterine pregnancy and is a medical emergency.
What are the alternatives?
If you’ve had a tubal ligation, in vitro fertilization (IVF) is an alternative path to pregnancy. IVF involves retrieving eggs, fertilizing them with sperm in a laboratory, and transferring resulting embryos directly into the uterus; if implantation succeeds, the pregnancy proceeds as usual.
Deciding between tubal reversal and IVF depends on individual factors. Evidence suggests IVF may be a better option for people over 40, while tubal reversal is often preferable for those under 40.
Cost is another consideration. For people under 40, reversal often ends up less expensive overall, including the subsequent costs of pregnancy. For those over 40, IVF may be more cost-effective. Pregnancy likelihood after each approach also varies by age: for women over 40, reversal yields about half the pregnancy rate of IVF; for women under 35, reversal often produces nearly double the pregnancy chances compared with IVF. For ages 35 to 40, pregnancy rates also tend to favor tubal reversal over IVF.
Bottom line
Tubal ligation reversal can make natural conception possible, but success depends on many factors — including age, the type of prior sterilization, the amount of healthy tube remaining, overall fertility, and cost considerations. Discuss your personal situation and options with your doctor to determine the best route to pregnancy.




















Leave a Reply
You must be logged in to post a comment.