
Neurologist Dr. Susan Lee addresses frequently asked questions about emerging migraine therapies and discusses where scientific advancements may lead in the coming years. As interest grows around treatment comparisons such as Nurtec vs Ubrelvy effectiveness, many patients are seeking clearer guidance on how newer options fit into today’s migraine care landscape.
What are the current options for treating or preventing migraine?
Conventional therapies taken at the beginning of a migraine attack (often referred to as acute or abortive treatment) typically involve oral medications, including:
- over-the-counter analgesics (pain relievers), such as aspirin, ibuprofen (Advil, Motrin IB), and acetaminophen (Tylenol)
- triptans, such as sumatriptan (Imitrex) and rizatriptan (Maxalt)
- ergots, such as dihydroergotamine (DHE-45, Migranal)
- anti-nausea medications, such as metoclopramide (Reglan, Metozolv ODT) and ondansetron (Zofran, Zofran ODT, Zuplenz)
Historically, preventive migraine medications were drugs originally developed for other health conditions but later found to reduce migraine frequency. These include:
- anti-hypertensives, such as propranolol (Hemangeol, Inderal, InnoPran XL) and verapamil (Calan, Calan SR, Verelan)
- antiseizure drugs, such as topiramate (Topamax, Eprontia) and valproate (Depakene, Depakote, Stavzor)
- antidepressants, such as amitriptyline (Elavil, Vanatrip) and venlafaxine (Effexor, Venbysi XR)
Botox injections received Food and Drug Administration (FDA) approval for chronic migraine in 2010, offering an additional preventive strategy for patients experiencing frequent headache days.
What are the latest developments in migraine care and treatment?
It is an especially promising era in migraine management due to the arrival of migraine-specific therapies. Unlike older medications, these treatments are designed to act on defined biological pathways involved in migraine pathophysiology.
In recent years, several innovative options have become available, including:
- calcitonin gene-related peptide (CGRP) antagonists
- lasmiditan
- neuromodulating devices
The introduction of the first CGRP antagonist, erenumab (Aimovig), marked a significant breakthrough. CGRP antagonists were the first migraine-specific medications approved since the development of triptans in the early 1990s.
CGRP antagonists include:
- injectable medications for preventive treatment, such as erenumab, galcanezumab-gnlm (Emgality), fremanezumab (Ajovy), and eptinezumab-jjmr (Vyepti)
- oral medications for acute treatment, such as ubrogepant (Ubrelvy) and rimegepant (Nurtec)
- oral medication for migraine prevention, such as rimegepant and atogepant (Qulipta)
These agents are distinctive not only for their targeted mechanism but also for the variety of administration methods available.
Lasmiditan (Reyvow) is a serotonin 5-HT1F receptor agonist approved for the acute treatment of migraine.
Neuromodulating devices work by stimulating specific nerves believed to play a role in migraine pain transmission. They may be used during an attack or as ongoing preventive therapy. Examples include:
- GammaCore
- Cefaly
- Nerivio
- Relivion
- sTMS mini (single-pulse transcranial magnetic stimulation)
Are there new preventive treatments for migraine? How do they compare to older treatments?
Newer preventive options include injectable CGRP antagonists (erenumab, galcanezumab-gnlm, fremanezumab-vfrm, and eptinezumab-jjmr) as well as the oral gepant atogepant (Qulipta). These therapies have expanded choices for individuals who cannot tolerate or do not respond to traditional preventive medications.
Clinical studies indicate that these treatments generally have a favorable side effect profile, including reassuring cardiovascular safety data.
At this time, no definitive head-to-head trials directly compare the efficacy of these newer agents with older preventive medications.
However, eptinezumab-jjmr has demonstrated effectiveness in migraine prevention beginning on day 1 of administration and sustained benefit over 12 to 18 months of therapy.
For patients weighing options, understanding differences in response rates, side effects, and practical considerations—such as insurance coverage and Nurtec vs Ubrelvy cost—can be just as important as comparing clinical outcomes.
Are there new acute treatments for migraine? How do they compare to older treatments?
The most recent acute migraine therapies include the CGRP antagonists ubrogepant, rimegepant (which carries dual approval for both acute and preventive treatment), and zavegepant (Zavzpret).
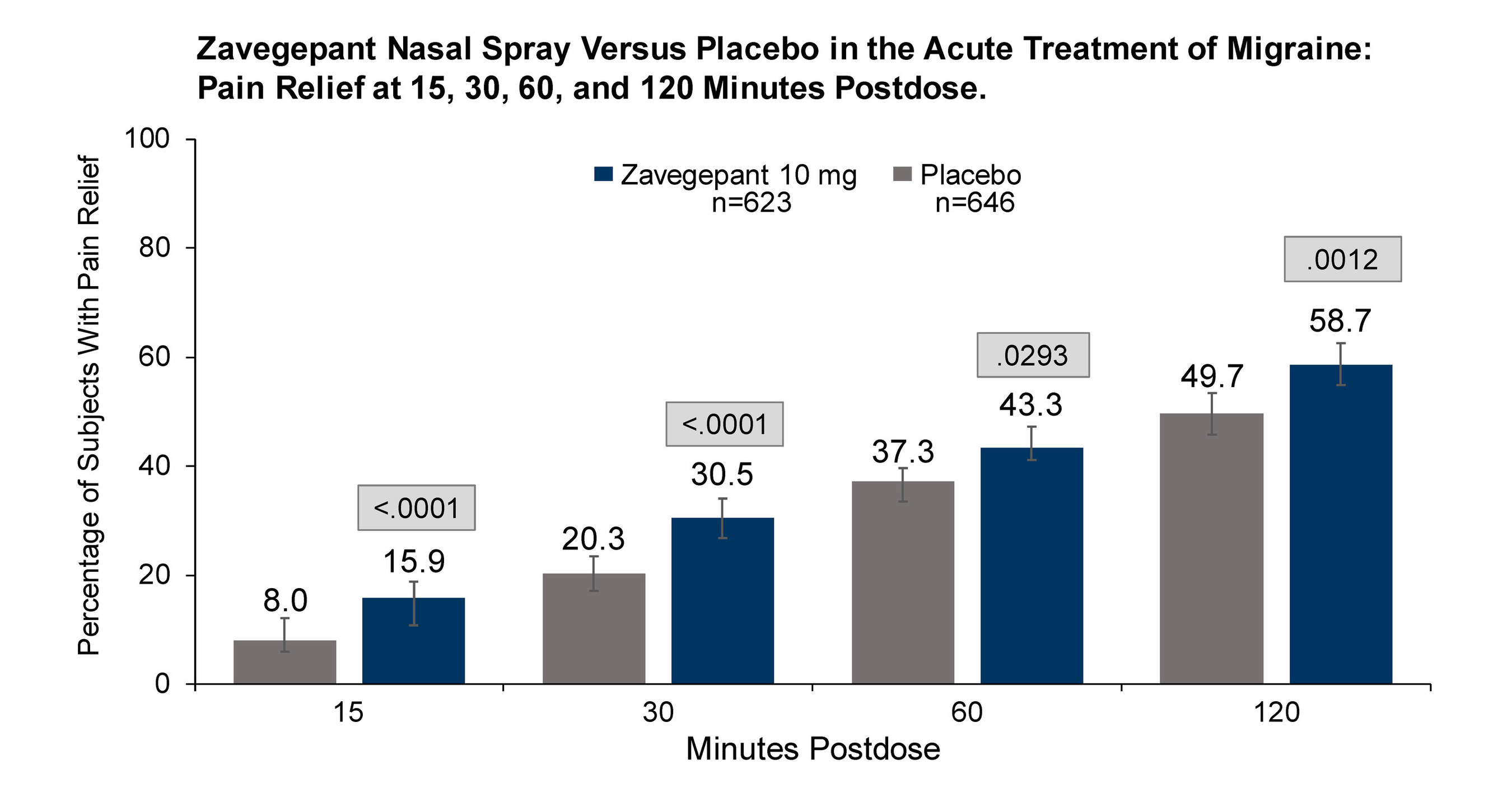
These medications have demonstrated a favorable side effect profile and have not been associated with increased cardiovascular or bleeding risk, which may occur with some older therapies such as triptans or nonsteroidal anti-inflammatory drugs. This distinction is often central to discussions about Nurtec vs Ubrelvy effectiveness, particularly for patients with cardiovascular risk factors.
Lasmiditan (Reyvow) is also effective for acute migraine and is considered safe in individuals with cardiovascular disease. However, it is known to cause dizziness and driving impairment.
Because of this effect, patients taking lasmiditan should avoid driving or operating hazardous machinery for at least 8 hours after a dose.
When comparing newer oral gepants, some patients and clinicians also explore broader comparisons such as Nurtec vs Ubrelvy vs Qulipta to better understand differences in preventive and acute indications.
What is CGRP? How is research on CGRP changing migraine treatment?
CGRP stands for calcitonin gene-related peptide. It is a neuropeptide released from nerves and blood vessels and is found to be elevated during migraine attacks, contributing to pain signaling.
Identifying CGRP’s involvement in migraine has transformed therapeutic development. CGRP antagonists work by blocking the action of CGRP, thereby reducing migraine symptoms or preventing attacks from occurring.
Ongoing research continues to evaluate various CGRP-targeted therapies, including:
- monoclonal antibodies, including: erenumab galcanezumab-gnlm fremanezumab eptinezumab-jjmr
- small, gepant molecules, including: ubrogepant rimegepant atogepant zavegepant
This expanding class of medications has redefined expectations for both acute relief and long-term migraine prevention.
Are there new delivery systems for migraine treatments? How do they affect treatment?
Modern migraine therapies now come in multiple delivery formats, such as:
- at-home injections, such as erenumab, galcanezumab-gnlm, fremanezumab (Ajovy)
- orally disintegrating tablets (rimegepant)
- IV infusions (eptinezumab-jjmr)
- intranasal sprays (zavegepant)
Neuromodulating devices may be:
- worn on or around the head (Cefaly, Relivion)
- worn around the arm (Nerivio)
- placed at the back of the head (sTMS)
- used as a stimulator to the neck (Gammacore)
A transdermal patch device (Zecuity) was previously marketed but later withdrawn because of safety concerns.
The availability of diverse administration routes enables clinicians and patients to tailor treatment based on migraine patterns, comorbidities, lifestyle factors, and personal preferences.
How might research into migraine biomarkers affect migraine management and treatment?
Discovering reliable migraine biomarkers could significantly enhance diagnostic accuracy. At present, migraine remains a clinical diagnosis based on symptom criteria.
If validated biomarkers become available, they could allow for earlier detection and more individualized therapy. Targeting specific biological markers may also support personalized migraine management strategies tailored to each patient’s unique disease profile.
Future treatments are likely to incorporate biomarker-driven approaches to improve precision and outcomes.
What is the latest research on lifestyle changes for migraine?
Research on lifestyle interventions for migraine frequently centers on sleep optimization, stress management, and nutraceuticals (foods or supplements that may provide health benefits beyond basic nutrition).

Wearable technology now allows individuals to monitor sleep patterns and identify potential migraine triggers. Smartphone applications also enable patients to log migraine episodes, track medication use, and access stress-reduction tools such as meditation and cognitive behavioral therapy (CBT).
Interest in nutraceuticals as a complementary or “natural” migraine strategy continues to grow, supported by expanding clinical data. These approaches may serve as adjuncts to pharmacologic therapy rather than replacements.
What areas might future migraine research focus on? Are we close to a cure for migraine?
Personalized medicine is expected to play an increasingly important role in migraine care. Ideally, treatment plans would be customized according to an individual’s symptom profile, genetic background, and coexisting medical conditions.
Another less common but evolving area is surgical intervention, including nerve decompression surgery or implantation of a neurostimulation device.
Further investigation is needed to confirm the safety and effectiveness of these surgical approaches. Although a definitive cure for migraine does not yet exist, the rapid expansion of targeted therapies and ongoing research offer meaningful hope for improved management and long-term relief.






















Leave a Reply
You must be logged in to post a comment.