
Hey there, friend. If you’ve ever felt a sudden, electric‑shock‑like jolt in your cheek, jaw or around your eye, you’re probably wondering “Is this trigeminal neuralgia or something else?” You’re not alone—many people wrestle with that exact question. Below you’ll get the straight‑forward, step‑by‑step rundown of how doctors pin down a trigeminal neuralgia diagnosis, how they sort it out from dental pain, TMJ syndrome or other headache causes, and what happens after the diagnosis is set. Grab a cup of tea, settle in, and let’s walk through this together.
Why Diagnosis Matters
Getting the right label on your facial pain is more than just semantics. A missed or delayed trigeminal neuralgia diagnosis can mean months of unnecessary dental work, lingering anxiety, and a longer road to effective relief. On the flip side, an early, spot‑on diagnosis opens the door to treatments that can tame the pain before it hijacks your daily life.
What are the risks of a missed or delayed diagnosis?
Imagine you’ve been to three dentists, had a root canal, and still feel that “sharp sting” every time you brush your teeth. That’s a story that pops up a lot. One real‑world case I read about involved a woman who waited three years before the correct diagnosis; by then she had developed secondary nerve damage that made treatment trickier. Studies from NYU Langone suggest up to 40 % of patients are first misdiagnosed as having a dental problem.
Benefits of an early, accurate diagnosis
- Targeted medication can start sooner, slashing the “electric” episodes.
- You avoid unnecessary dental procedures, saving time, money, and hassle.
- A clear plan lets you and your doctor discuss long‑term options—whether medication, minimally invasive injections, or surgery.
Mimicking Conditions
Facial pain loves to play hide‑and‑seek. Below is a quick‑glance table that shows why it’s easy to confuse trigeminal neuralgia with other culprits.
| Condition | Typical Pain Pattern | Key Red‑Flag Differences | When to Refer |
|---|---|---|---|
| Dental pain / tooth infection | Localized to one tooth; worse with biting | Positive dental X‑ray; often resolves after dental treatment | Immediate dentist |
| TMJ syndrome | Jaw ache, clicking, morning stiffness | Joint sounds, limited mouth opening, pain worsens with chewing | Dentist or oral‑maxillofacial specialist |
| Cluster headache | Unilateral orbital pain, lasting 15‑180 min, with tearing | Autonomic signs (red eye, nasal congestion) and seasonal pattern | Neurologist |
| Post‑herpetic neuralgia | Burning after shingles, follows dermatome | History of shingles, visible skin lesions | Dermatology or Neurology |
| Sinusitis / other headaches | Pressure‑like ache, nasal congestion, possible fever | Congestion, sinus tenderness, imaging shows sinus blockage | ENT specialist |
When you compare this table to your own symptoms, you’ll often see a pattern that leans toward trigeminal neuralgia—especially if the pain is brief, shock‑like, and triggered by everyday actions like brushing or smiling.
Diagnostic Steps
1️⃣ Detailed Clinical Interview
First thing the doctor will do is ask you to paint a vivid picture of your pain. Think of it like a detective interview:
- When did it start? Sudden vs. gradual.
- How long does each episode last? Seconds, minutes, or longer?
- How often? A few times a day or dozens of attacks?
- What triggers it? Chewing, wind, cool breezes, talking, shaving.
- How would you describe it? “Electric shock,” “stabbing,” “sharp” are the classic words.
This “patient‑pain questionnaire” is the backbone of a solid trigeminal neuralgia diagnosis. If you can answer these questions clearly, you’re already helping the clinician a lot.
2️⃣ Focused Neurological Examination
Next up, the doctor will test the three branches of the trigeminal nerve (ophthalmic, maxillary, mandibular). They’ll gently touch the skin, ask you to feel cotton wools, and check for any numbness or weakness. The exam is usually normal in classic TN, but any sensory loss or bilateral pain points toward a secondary cause.
3️⃣ Dental & TMJ Screening
Because dental pain is a top mimic, a quick dental X‑ray (often a panoramic view) is ordered. The dentist also looks for cracked teeth, abscesses, or bite misalignments. If nothing shows up, they’ll signal the need for a neurologic work‑up.
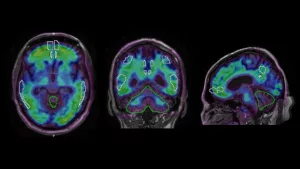
4️⃣ Imaging & Ancillary Tests
Imaging is the crown jewel for confirming the diagnosis and ruling out other scary stuff.
| Test | What It Shows | Typical TN Findings | When It’s Recommended |
|---|---|---|---|
| MRI of brain & cranial base (high‑resolution) | Soft‑tissue anatomy, nerve‑vascular relationships | Blood‑vessel loop touching the trigeminal root; sometimes MS plaques | First‑line when TN is suspected |
| MR Angiography (MRA) | Detailed vascular map | Identifies offending artery (e.g., AICA) | If MRI inconclusive or for surgical planning |
| CT scan | Bone & sinus structures | Excludes sinus disease, dental pathology | When MRI unavailable or contraindicated |
| Electrophysiological studies (blink reflex) | Neural conduction | Abnormal latency in TN | Rare, used in specialized centers |
According to the NHS, MRI is the gold standard—it can spot the exact vessel compressing the nerve and differentiate classical TN from secondary causes like tumors.
5️⃣ Differential Diagnosis Confirmation
Once the interview, exam, and imaging line up, doctors use a decision‑tree flowchart:
- Typical shock‑like pain + normal neuro exam → Clinical suspicion of TN
- Positive MRI showing neurovascular contact → Classical TN confirmed
- No contact but symptoms fit → Atypical/secondary TN (needs further work‑up)
- Red‑flag findings (sensory loss, bilateral pain, visual changes) → Refer for urgent neuro‑imaging and possibly neurosurgery
Red Flag Signs & When to Seek Immediate Care
Even though TN isn’t usually life‑threatening, certain symptoms scream “call the doctor right now”.
- Sudden loss of facial sensation or strength.
- Persistent, unrelenting pain that doesn’t respond to medication.
- Vision changes, hearing loss, or facial droop.
- Severe headache that’s new or worsening.
These could signal a tumor, stroke, or aneurysm—conditions that demand fast action.
Understanding Test Results
MRI evidence of neurovascular compression
When the MRI shows an artery (often the anterior inferior cerebellar artery) pressing against the trigeminal root, it’s called “vascular loop compression”. This is the hallmark of classical TN and often guides surgeons toward a microvascular decompression (MVD) procedure.
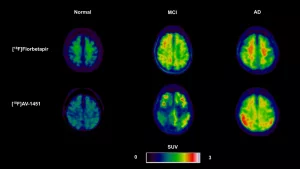
Multiple‑Sclerosis plaques
If the MRI reveals demyelinating plaques in the brainstem, the diagnosis shifts toward secondary TN caused by MS. Treatment then incorporates disease‑modifying therapies for MS alongside pain control.
Absence of structural cause
When imaging is clean but the symptoms fit, doctors label it “classical” TN. It’s a diagnosis of exclusion, but the good news is that the typical medication regimen works well for most patients.
After the Diagnosis – Treatment Paths
Now that the label is on the board, let’s talk about what comes next. Treatment is stepped, starting with the least invasive.
| Treatment | First‑line? | Typical Success Rate | Common Side‑effects | When Considered |
|---|---|---|---|---|
| Carbamazepine (anti‑seizure) | Yes | 70‑80 % | Dizziness, rash, blood‑test monitoring | All newly diagnosed patients |
| Oxcarbazepine, Gabapentin, Pregabalin | Alternative | 60‑70 % | Sedation, weight gain | If carbamazepine intolerable |
| Microvascular Decompression (MVD) | Surgical | 80‑90 % (long‑term) | CSF leak, infection, hearing loss | Vascular compression confirmed, meds fail |
| Radiofrequency Ablation / Glycerol Injection | Minimally invasive | 50‑70 % | Facial numbness, rare dysesthesia | Medication ineffective or side‑effects |
| Botulinum toxin injections | Emerging | 50‑60 % | Temporary weakness, injection site pain | Focal attacks, patient preference |
Guidelines from Mayo Clinic emphasize starting with carbamazepine and moving up the ladder only when needed.
Living With a Trigeminal Neuralgia Diagnosis – Risks & Benefits
Managing medication risks
Carbamazepine requires blood‑test monitoring for liver function and blood counts, especially in the first few months. If you’re of Asian descent, a genetic test for HLA‑B*1502 is often recommended to avoid a rare but serious skin reaction.
Lifestyle adjustments
- Adopt a soft‑food diet during flare‑ups—think oatmeal, smoothies, scrambled eggs.
- Keep a “trigger journal” to spot patterns (e.g., cold wind, chewing gum).
- Practice stress‑reduction techniques—deep breathing or gentle yoga can lower attack frequency.
- Use a warm compress on the cheek during an episode; many find it soothing.
Psychological impact & support
Living with unpredictable pain can feel isolating. It’s normal to develop anxiety or avoid social situations. Talking to a therapist, joining a patient‑support group, or even sharing your story on a forum can make a huge difference. The Trigeminal Neuralgia Association UK offers online meet‑ups that many find comforting.
Follow‑up schedule
After the initial diagnosis:
- First medication review at 2‑4 weeks.
- Neurological exam every 6‑12 months.
- Repeat MRI if symptoms change or after 2‑3 years of stable disease (helps catch any new compression).
- Prompt reassessment if red‑flag signs appear.
Expert Sources & Further Reading
Building trust means leaning on solid, peer‑reviewed data:
- National Health Service (NHS) – detailed diagnostic pathway.
- NYU Langone – clinical experience with neurovascular imaging.
- Mayo Clinic – medication and surgical options.
- British NICE Clinical Knowledge Summaries – evidence‑based guidelines.
- BMJ Open Practice article “Practical Guide to Trigeminal Neuralgia” (2021) for in‑depth expert insights.
Takeaway
Getting a clear trigeminal neuralgia diagnosis is a journey that starts with a simple yet precise conversation about your pain, followed by a focused exam, smart imaging, and a careful ruling‑out of dental, TMJ or other headache causes. When the diagnosis lands, you have a menu of proven treatments—starting with medication and moving up to minimally invasive procedures or surgery if needed. Early identification means quicker relief, fewer unnecessary procedures, and a better quality of life.
Do you recognize any of these patterns in your own experience? Have you already been on this diagnostic road and want to share what helped you the most? Drop a comment below, or reach out to a trusted clinician. Remember, you’re not alone, and the right diagnosis is the first step toward getting your life back under control.





















Leave a Reply
You must be logged in to post a comment.