
A fenestrated tracheostomy tube includes an extra opening that can provide more function than a tube without one, but it also brings added hazards.
A tracheostomy is an operation to make an opening in the neck that leads to the trachea, or windpipe. The words “tracheostomy” and “tracheotomy” are frequently used synonymously; here we’ll use “tracheostomy.”
There are many reasons someone might require a tracheostomy. It’s typically a planned operation performed under general anesthesia, though in emergencies a related but different procedure called a cricothyrotomy may be done.
A tracheostomy may be necessary if the upper airway is obstructed or injured, or if you cannot protect your lungs from aspiration of fluids.
The procedure creates an opening, or stoma, into the trachea below the vocal cords. A tube is placed into the stoma so air can reach your lungs without traveling through the nose or mouth.
That tube may be either fenestrated or non-fenestrated. A fenestrated tube has an extra aperture that can increase functionality but may also introduce particular risks.
Below we’ll explore fenestrated tracheostomy tubes in more detail.
When are fenestrated tracheostomy tubes used?
After a tracheostomy, the tube might be temporary. In other situations—such as significant irreversible damage to the upper airway—a permanent tracheostomy tube may be required. The choice largely depends on the reason for the tracheostomy and the patient’s overall condition.
Whether temporary or permanent, tracheostomy tubes need routine cleaning and occasional replacement.
If your tracheostomy is temporary, you may be transitioned to a fenestrated tracheostomy tube as you recover.
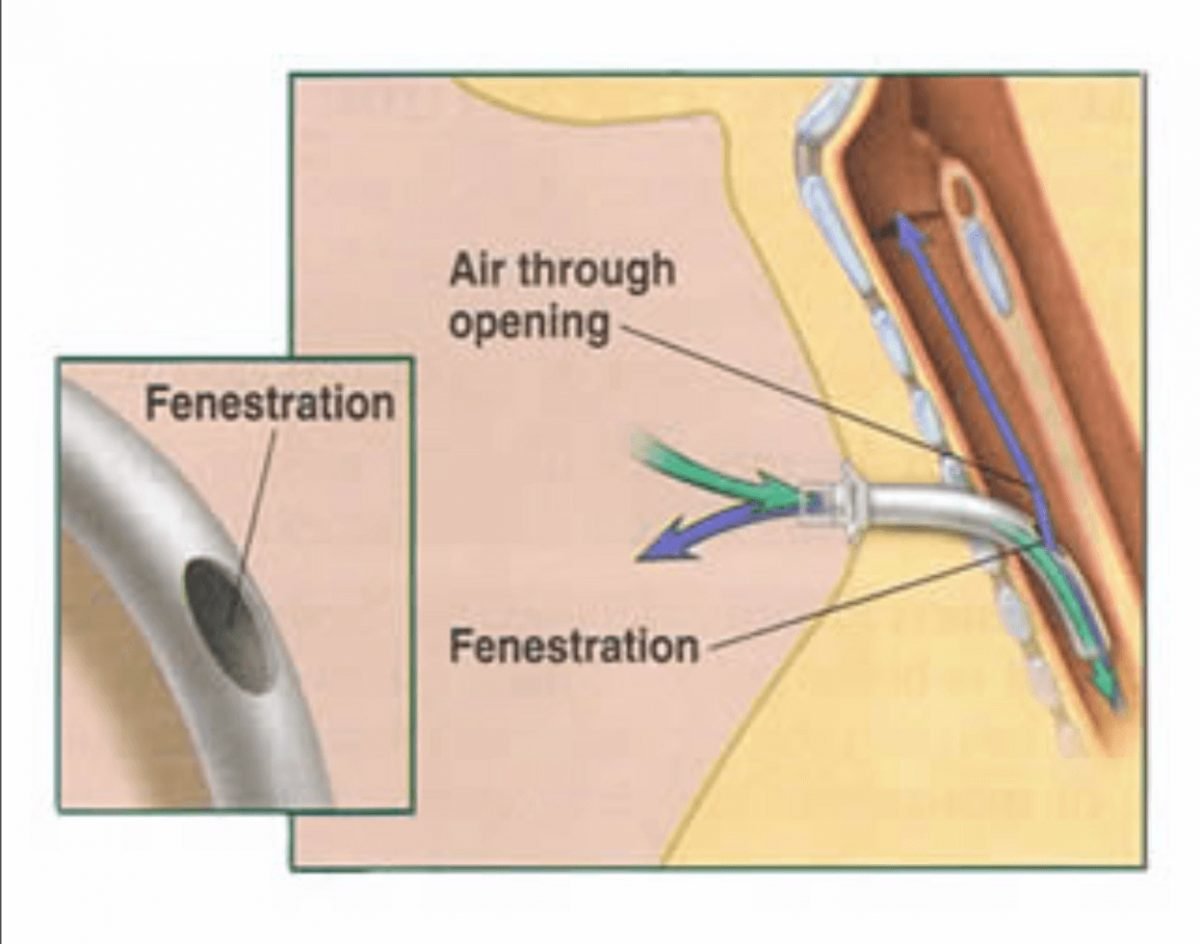
The fenestration allows exhaled air to flow into the throat and out through the nose or mouth, which can enable speech. It can also reduce the effort of breathing, which is helpful when weaning from a ventilator (extubation).
Fenestrated vs non-fenestrated tracheostomy tubes
Around the exterior of many tracheostomy tubes is a small inflatable cuff. When inflated, this cuff seals the trachea so that airflow to and from the lungs only occurs through the tube.
The cuff helps keep secretions such as saliva from entering the lungs, but it also blocks air from passing over the vocal cords, preventing speech.
In some situations, speaking is possible with the cuff deflated, but this is often difficult or unachievable.
A fenestrated tracheostomy tube contains one or more small openings—fenestrations—that permit exhaled air to travel over the vocal cords so the person can speak.
A non-fenestrated tracheostomy tube lacks these openings, making speech unlikely. An alternative is a speaking valve, an attachment placed on the tube’s end to facilitate vocalization, though not everyone adapts easily to it. For more detailed comparisons, see laryngectomy tube vs tracheostomy tube.
Risks associated with fenestrated tracheostomy tubes
Fenestrated tracheostomy tubes are linked with specific potential complications.
Because of the fenestrations, secretions or food particles can more readily enter the tube. Debris inside the tube can partly or completely obstruct airflow to the lungs. Material may also travel down the tube and enter the lungs, causing additional problems.
Cleaning a fenestrated tube can be riskier as well. Tracheostomy tubes require periodic clearing with a specialized suction device. With a fenestrated tube, there’s a possibility the suction catheter could pass through a fenestration and injure the adjacent tracheal tissues.
For these reasons, clinicians commonly place a non-fenestrated tube immediately after surgery. A fenestrated tube may be considered later as recovery progresses.

Recovering after a tracheostomy
Recovery varies by individual based on health status and the reason for the tracheostomy. The stoma itself usually heals within about a week.
The area around the stoma must be kept clean. If your condition allows, you may be able to eat with a tracheostomy tube in place. You may be advised to avoid heavy physical exertion for one to two months following the operation.
Discussing recovery expectations with your doctor can help you plan and understand likely outcomes.
Takeaway
Following a tracheostomy, a tube is inserted into the stoma to allow air to move in and out of the lungs.
Tracheostomy tubes may be fenestrated or non-fenestrated. A fenestrated tube has openings that can make speaking easier, but those openings can introduce additional risks.
If you are scheduled for a tracheostomy, talk with your healthcare provider about which type of tube they plan to use and why.




















Leave a Reply
You must be logged in to post a comment.