
Subclinical hyperthyroidism is identified when thyroid-stimulating hormone (TSH) levels are low or undetectable, while circulating thyroid hormones remain within the normal laboratory range. In many cases, individuals have no noticeable symptoms, and treatment may not be immediately necessary.
Hyperthyroidism develops when the thyroid gland produces excessive amounts of the hormones T3 and T4. In response, the pituitary gland senses this increase and decreases TSH production in an effort to lower T3 and T4 levels.
Physicians typically diagnose overt hyperthyroidism when blood tests reveal elevated T3 and T4 levels alongside reduced TSH.
In subclinical hyperthyroidism, T3 and T4 concentrations are still within standard reference ranges, but TSH levels are suppressed. This indicates that the body is attempting to limit thyroid hormone production despite laboratory values appearing normal for T3 and T4.
Subclinical thyroidism is often regarded as a milder or early stage form of hyperthyroidism.
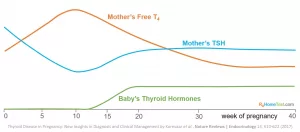
Accurate thyroid assessment becomes particularly important during pregnancy. Tests such as the tsh w/reflex to ft4 pregnancy panel help clinicians interpret hormone fluctuations appropriately. Understanding the TSH W reflex to FT4 pregnancy reference range ensures that normal pregnancy-related hormonal changes are not mistaken for pathology. In some cases, a TSH w reflex to ft4 pregnancy test is ordered to automatically measure FT4 when TSH results fall outside expected limits.

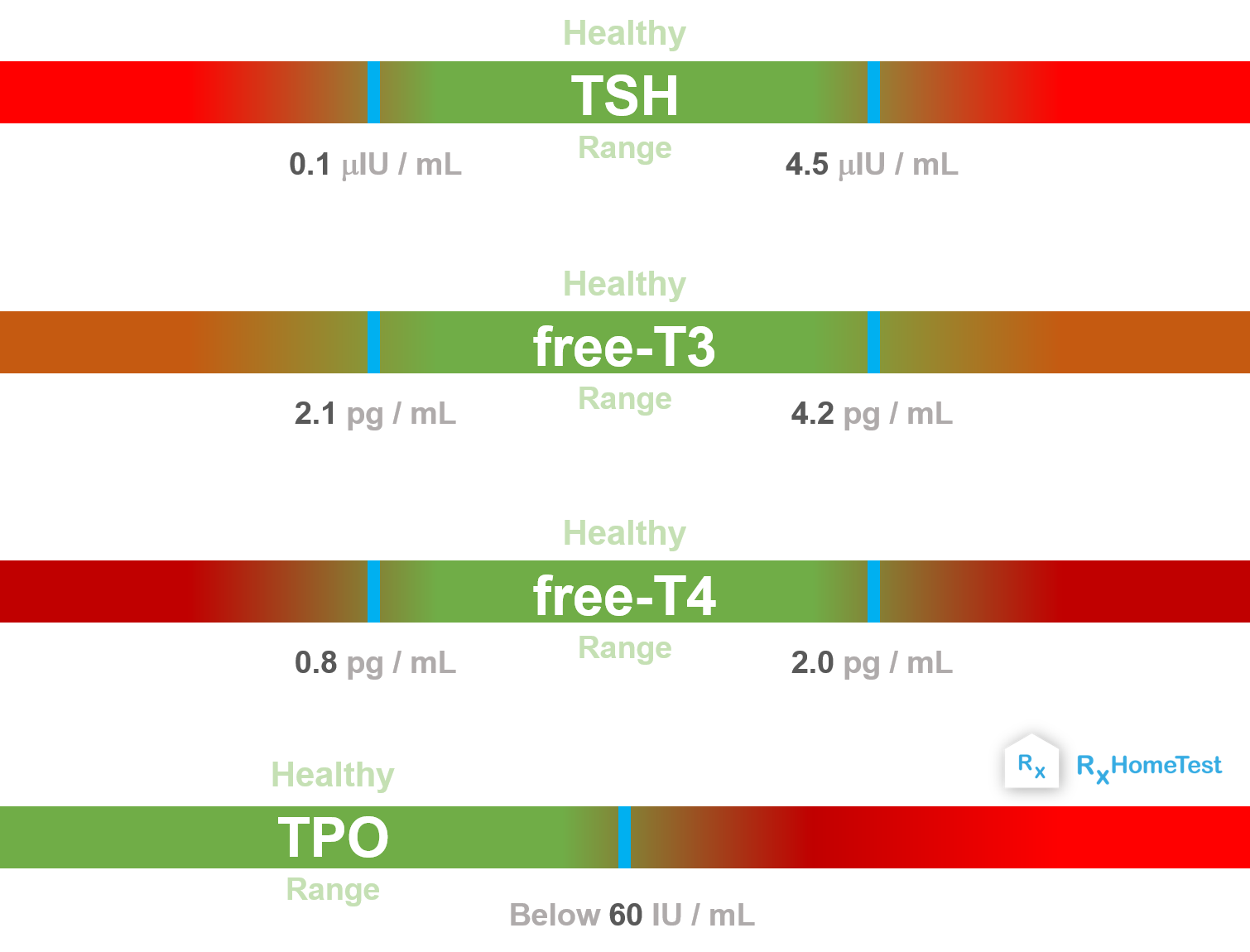
- T4 (thyroxine) is a primary hormone released by the thyroid gland. It is considered inactive until converted.
- T3 (triiodothyronine) is the active form of T4. The body transforms T4 into T3 to exert metabolic effects.
- TSH is secreted by the pituitary gland and regulates T4 production. When the pituitary senses low T4 levels, it increases TSH output, stimulating the thyroid to release more T4. Conversely, when T4 levels are high, TSH secretion decreases, reducing further thyroid hormone production.
What are the symptoms?
Most individuals with subclinical hyperthyroidism do not exhibit obvious signs of an overactive thyroid. When symptoms do occur, they are generally mild and nonspecific, which can make recognition challenging.
Possible symptoms include:
- fast heartbeat or heart palpitations
- trembling, often in the hands or fingers
- excessive sweating or sensitivity to heat
- nervousness, anxiety, or irritability
- unintentional weight loss
- trouble focusing or concentrating
If you suspect you may be experiencing symptoms consistent with subclinical hyperthyroidism, consult your healthcare provider for appropriate evaluation and thyroid function testing.
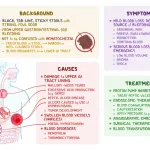
Common causes
Subclinical hyperthyroidism may arise from endogenous (internal) or exogenous (external) causes.
Internal causes
Internal factors that may contribute to subclinical hyperthyroidism include:
- Graves’ disease. Graves’ disease is an autoimmune disorder that triggers excessive production of thyroid hormones.
- Multinodular goiter. A goiter refers to an enlarged thyroid gland. A multinodular goiter contains multiple nodules within the enlarged gland.
- Thyroiditis. Thyroiditis involves inflammation of the thyroid gland and encompasses several related conditions.
- Thyroid adenoma. A thyroid adenoma is a benign tumor of the thyroid gland.
External causes
External contributors to subclinical hyperthyroidism may include:
- excessive TSH-suppressive therapy
- accidental TSH suppression during hormone replacement therapy for hypothyroidism
Subclinical hyperthyroidism can also develop during pregnancy, especially in the first trimester. Importantly, it is not associated with adverse pregnancy outcomes and generally does not require treatment. Clinicians rely on pregnancy-specific laboratory standards, including the TSH W reflex to FT4 pregnancy reference range, to distinguish normal physiologic changes from thyroid dysfunction.
How it’s diagnosed
If subclinical hyperthyroidism is suspected, your doctor will first measure your TSH level through a blood test.
When TSH is found to be low, additional testing is performed to evaluate T4 and T3 levels to determine whether they remain within normal limits.
These evaluations require a simple blood sample, typically drawn from a vein in your arm.
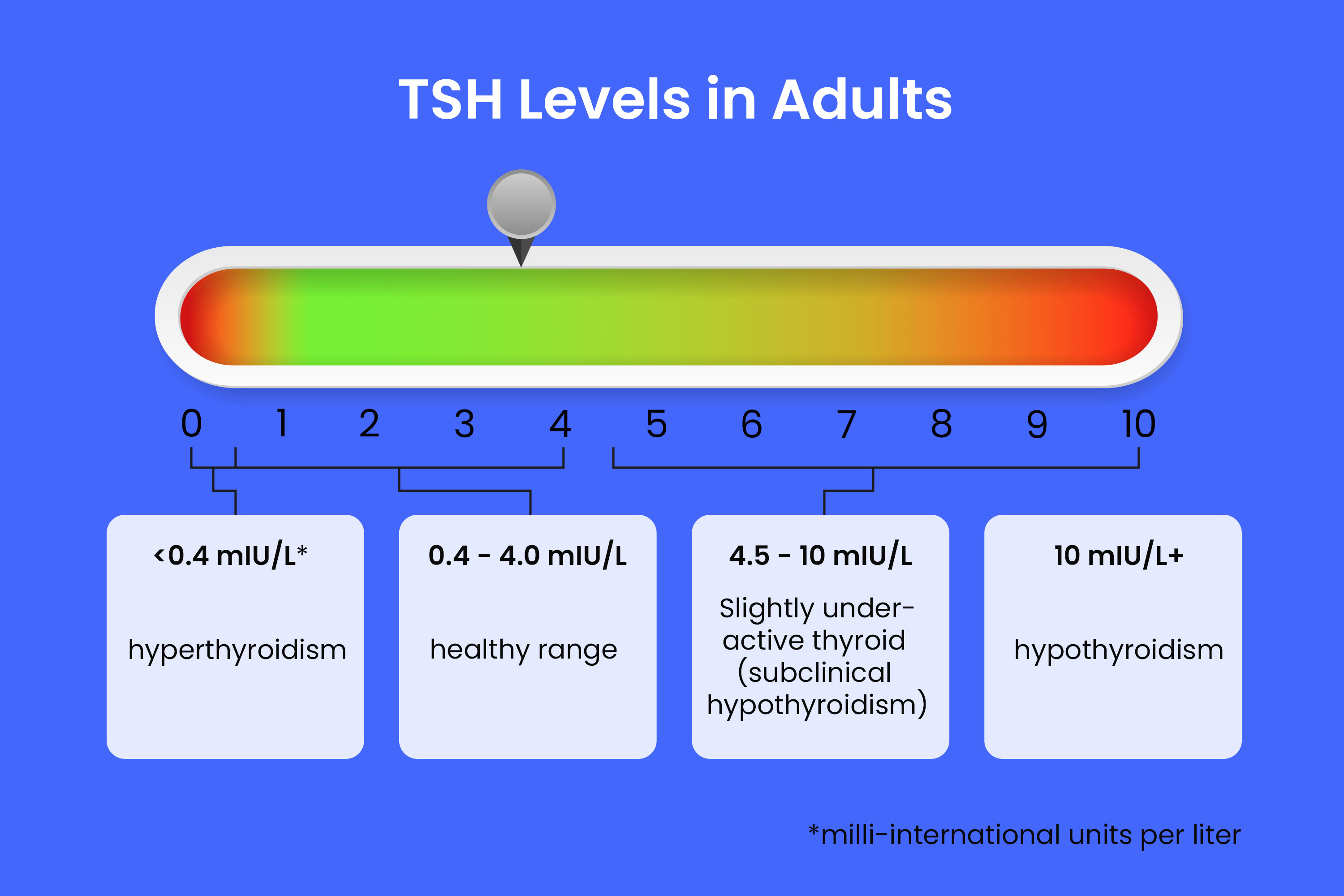
According to the American Thyroid Association, the standard reference range for TSH in adults is generally 0.4 to 4.0 milli-international units per liter (mIU/L). However, always refer to the specific reference values provided by your laboratory, as ranges can vary.
Subclinical hyperthyroidism is commonly divided into two categories:
- Grade I: Low but detectable TSH, typically between 0.1 and 0.4 mIU/L.
- Grade II: Undetectable TSH, defined as less than 0.1 mIU/L.
In pregnancy, interpretation of results requires trimester-specific adjustments. Using panels such as the TSH w/reflex to FT4 pregnancy assessment helps ensure that FT4 is measured automatically if TSH falls outside expected pregnancy norms.
Treatment
A 2018 review of scientific studies reported that mildly decreased TSH levels frequently normalize without intervention.
However, subclinical hyperthyroidism may sometimes contribute to:
- Increased risk of hyperthyroidism. Individuals with undetectable TSH have a higher likelihood of progressing to overt hyperthyroidism.
- Negative cardiovascular effects. Untreated cases may result in increased heart rate, reduced exercise tolerance, arrhythmias, and atrial fibrillation.
- Decreased bone density. In postmenopausal women, untreated subclinical hyperthyroidism can lead to reduced bone mineral density.
The need for treatment depends on several factors:
- the underlying cause
- the degree of TSH suppression
- whether complications are present
Treating internal causes
If subclinical hyperthyroidism is caused by Graves’ disease, medical management is necessary. Treatment options may include radioactive iodine therapy or anti-thyroid medications such as methimazole.
Radioactive iodine and anti-thyroid drugs may also be used for subclinical hyperthyroidism resulting from multinodular goiter or thyroid adenoma.
When thyroiditis is responsible, the condition often resolves on its own without specific therapy. In more severe cases, anti-inflammatory treatment may be prescribed, including nonsteroidal anti-inflammatory drugs (NSAIDs) or corticosteroids.
Treating external causes
If subclinical hyperthyroidism results from TSH-suppressive therapy or hormone replacement therapy, your physician may adjust the medication dosage as needed.
Treatment based on severity
If TSH levels are low but still measurable and no complications are present, immediate treatment may not be required. Instead, your doctor may monitor TSH every few months until levels normalize or remain stable.
Treatment is more likely to be recommended if TSH levels fall into Grade I or Grade II and you:
- are older than 65
- have cardiovascular disease
- have osteoporosis
- experience symptoms consistent with hyperthyroidism
Your management plan will be tailored to the specific cause of your subclinical hyperthyroidism.
Treatment with complications
If cardiovascular or skeletal complications develop, medications such as beta-blockers for heart-related symptoms and bisphosphonates for bone protection may be beneficial.
Home treatment
Research suggests that potential negative effects on bone density may be mitigated by ensuring adequate daily calcium intake. Maintaining sufficient vitamin D levels may also support bone health, particularly in individuals at risk of osteoporosis.
Unintentional weight loss can occur in subclinical hyperthyroidism due to an elevated basal metabolic rate (BMR). A higher BMR means the body requires more calories to maintain its current weight. Paying attention to balanced nutrition and adequate caloric intake can help prevent excessive weight loss.
Takeaway
Subclinical hyperthyroidism is characterized by low TSH levels with normal T3 and T4 concentrations. If symptoms suggest thyroid imbalance, your healthcare provider can confirm the diagnosis through blood testing.
Because multiple factors can cause this condition, treatment decisions are guided by the underlying cause and the severity of hormone suppression. Once TSH levels return to normal—either spontaneously or with treatment—most individuals do not experience long-term consequences from subclinical hyperthyroidism.

















Leave a Reply
You must be logged in to post a comment.