
Key takeaways
- Graves’ disease is an autoimmune condition that causes hyperthyroidism, or excess thyroid hormone production. Persistently elevated thyroid hormone levels can gradually damage the heart, bones, skin, and eyes.
- Frequent complications include thyroid eye disease, osteoporosis, goiter, and cardiovascular issues such as arrhythmias. Treatment depends on the specific complication and may involve anti-thyroid drugs, beta-blockers, steroids, radiation, or surgery.
- Thyroid storm is a rare but life-threatening emergency marked by high fever and rapid heartbeat. Call 911 right away if these symptoms develop, and consult your doctor before pregnancy to reduce potential risks.
If you’ve been diagnosed with this condition, you may wonder how long can you live with graves’ disease. The reassuring answer is that with timely diagnosis, consistent monitoring, and appropriate treatment, most people can live a normal life expectancy. However, untreated or poorly controlled hyperthyroidism can result in serious health complications over time.
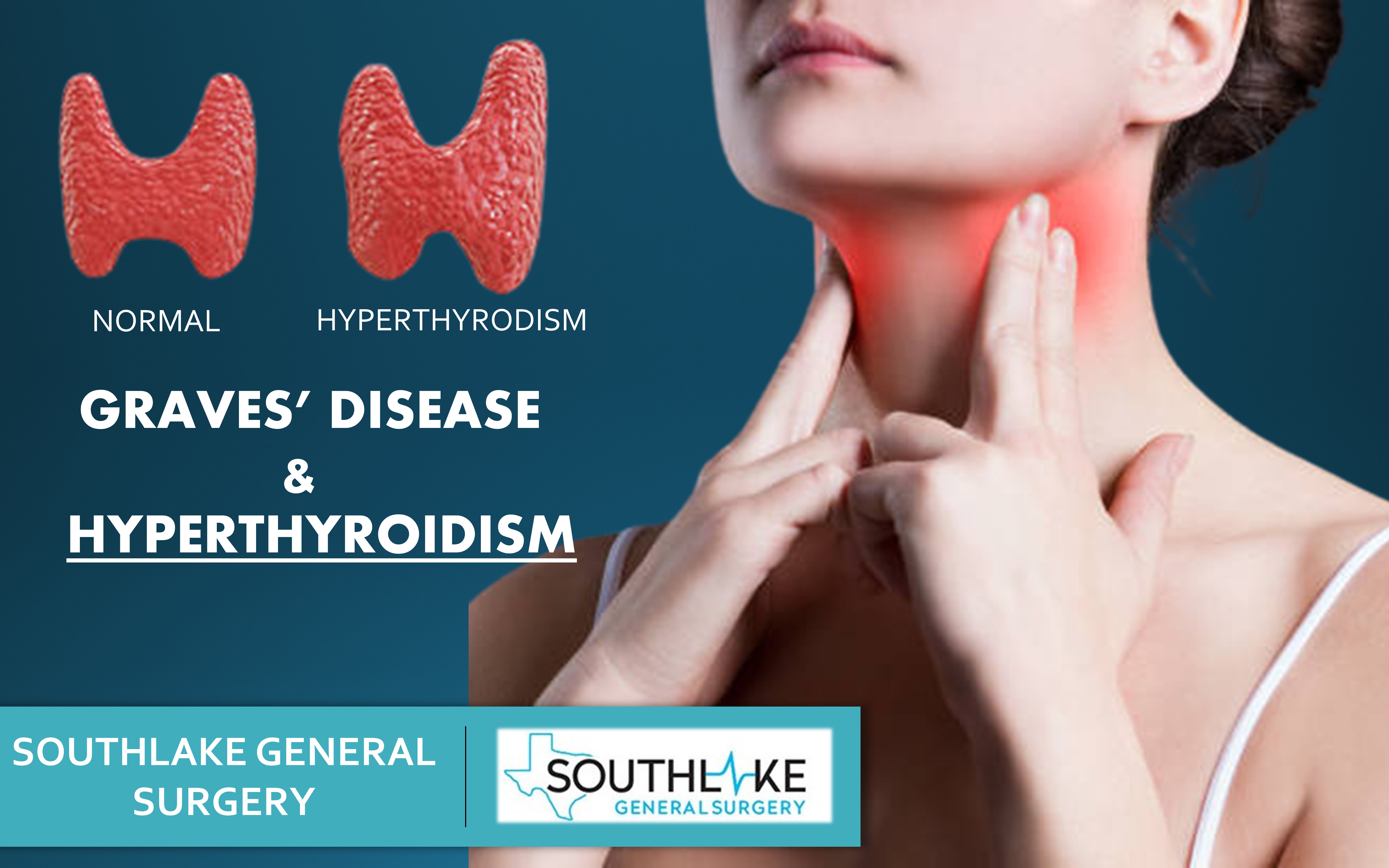
The thyroid gland, located at the base of your neck, produces hormones that regulate how your body uses energy. These hormones influence nearly every organ system, including the heart, brain, muscles, and bones.
Graves’ disease is an autoimmune disorder in which the immune system mistakenly attacks the thyroid gland, causing it to become overactive — a condition known as hyperthyroidism.
Many of the symptoms and long-term risks associated with Graves’ disease stem from excessive thyroid hormone production. Over time, and especially without proper treatment, the condition may lead to long-term effects involving the heart, skeletal system, skin, and eyes.
Below, we explore several potential complications of Graves’ disease, along with guidance on recognizing, preventing, and managing them. Understanding these risks can help answer concerns about long-term survival and quality of life.
Thyroid eye disease (TED)
Thyroid eye disease (TED) is an inflammatory condition affecting the tissues surrounding the eyes. It occurs when immune cells mistakenly target the fat and connective tissues within the eye socket. Graves’ disease is the number one cause of TED, which is why it’s often called:
- Graves’ orbitopathy
- Graves’ ophthalmopathy
- Graves’ eye disease
Common symptoms of TED include:
- protruding or bulging eyes
- swelling around the eyes
- eye irritation or redness
- retracted eyelids
- vision disturbances such as double vision or blurry vision
- light sensitivity
- eye misalignment
- permanent vision loss (rare)
Treatment options for TED may involve anti-inflammatory medications like steroids, the IV medication teprotumumab (Tepezza), or radiation therapy to reduce inflammation and swelling.
If you smoke, quitting is strongly recommended, as smoking can worsen TED symptoms and delay recovery. In cases involving lasting structural changes, surgical intervention may be necessary.
In many individuals, TED enters an inactive phase after 6 months to 2 years of treatment.
Osteoporosis
Thyroid hormones play a critical role in bone growth and bone remodeling.
According to the British Thyroid Foundation, excessive thyroid hormone — as seen in Graves’ disease — accelerates bone turnover, causing bone mass to decline and mineral density to drop. Over time, this can result in osteoporosis, a condition characterized by fragile bones and an increased fracture risk.
Osteoporosis often develops silently, without obvious early symptoms. As it advances, the likelihood of fractures — especially in the hips, spine, and wrists — increases.
While there’s no cure for osteoporosis, several treatments and lifestyle strategies can strengthen bones and reduce fracture risk. These include:
- bisphosphonates, such as alendronate (Fosamax) and ibandronate (Boniva)
- hormone therapy, including teriparatide (Forteo)
- biologics like denosumab (Prolia)
- calcium and vitamin D supplementation
- engaging in weight-bearing or high-impact exercises such as strength training, jogging, or stair climbing
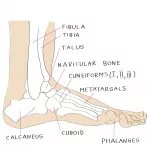
Skin problems
Graves’ disease may lead to thickened, reddish, and rough skin over the shins and tops of the feet. This condition is known as Graves’ dermopathy or pretibial myxedema.
This complication affects up to 3 in 100 people with Graves’ disease. Older research indicates it may occur in as many as 15% of people with severe Graves’ disease.
Although usually mild, it can cause discomfort or cosmetic concerns. Many cases resolve on their own, but topical steroids or steroid injections may be used if symptoms persist.
Heart problems
Excess thyroid hormone significantly impacts the cardiovascular system, increasing heart rate and cardiac output.
Over time, this heightened workload can strain the heart. If left unmanaged, Graves’ disease may contribute to heart failure and other serious complications, including:
- rhythm disorders (arrhythmias)
- rapid heartbeat (tachycardia)
- impaired pumping ability
- heart failure
- high blood pressure
- heart disease
- increased surgical risk
- blood clots
- stroke
Management depends on the specific cardiac issue. Beta-blockers are commonly prescribed to control heart rate, alongside anti-thyroid medications to regulate hormone levels. Addressing hyperthyroidism early plays a key role in protecting long-term heart health.
Thyroid storm
Thyroid storm, also called thyrotoxic crisis, is a rare but life-threatening escalation of hyperthyroidism caused by a sudden surge in thyroid hormones.
Symptoms may include:
- high fever
- excessive sweating
- fast heartbeat (tachycardia)
- vomiting
- diarrhea
- jaundice
- abdominal pain
- low blood pressure
- weakness
- delirium
- irregular heartbeat (arrhythmia)
- coma
Thyroid storm requires immediate treatment in an intensive care unit (ICU). If you have Graves’ disease and develop these symptoms, call 911 without delay.
Because thyroid storm can be fatal, many people researching how long can you live with graves’ disease are often reassured to learn that this complication is rare and largely preventable with proper treatment and monitoring.
Goiter
In Graves’ disease, overstimulation of the thyroid causes the gland to enlarge, producing visible swelling in the neck known as a goiter.
While often painless, a large goiter may cause:
- difficulty swallowing or breathing
- persistent coughing
- a choking sensation
- voice hoarseness
Anti-thyroid medications used to control hormone production may also reduce thyroid enlargement over time.
High risk pregnancy
Untreated Graves’ disease can increase the likelihood of pregnancy complications, including:
- miscarriage or stillbirth
- premature birth
- preeclampsia (high blood pressure)
- low birth weight
- intrauterine growth restriction (IUGR)
- placental abruption
- premature rupture of membrane
- birth defects
Research shows that maintaining stable, normal thyroid hormone levels throughout pregnancy significantly reduces these risks.
If you’re planning a pregnancy, consult your doctor in advance. Careful monitoring before and during pregnancy is essential for maternal and fetal health.
Blood problems
In rare cases, Graves’ disease may be associated with blood-related complications such as pancytopenia and agranulocytosis.
Pancytopenia
Pancytopenia is an uncommon condition characterized by low levels of red blood cells, white blood cells, and platelets.
Research indicates that hyperthyroidism in Graves’ disease may contribute to pancytopenia by:
- reducing production of new hemopoietic cells in the bone marrow
- increasing destruction of existing hemopoietic cells
Symptoms may include dizziness, fatigue, muscle weakness, difficulty breathing, tachycardia, fever, pale skin, easy bruising, and abnormal bleeding.
Treatment typically includes anti-thyroid medication to control the overactive thyroid.
Agranulocytosis
Thionamides, a class of drugs used to treat Graves’ disease, may lead to agranulocytosis. This condition occurs when granulocyte levels — a type of white blood cell — drop dangerously low.
Symptoms resemble those of pancytopenia and may include fever, chills, sore throat, mouth sores, bleeding in the mouth, bone pain, difficulty breathing, and tachycardia.
Seek immediate medical care if these symptoms appear, as agranulocytosis weakens the immune system and raises the risk of severe infection.
Preventing complications
Early diagnosis and consistent treatment greatly improve outcomes and help answer the common concern about how long can you live with graves’ disease. With proper management, most people live full, healthy lives.
You can reduce your risk of complications by:
- working closely with your doctor
- adhering to your prescribed treatment plan
- undergoing routine screenings, such as bone density and blood pressure checks
- taking medications and supplements as directed
- avoiding smoking
- managing stress
- engaging in regular physical activity, including weight-bearing exercise
- eating nutrient-rich foods high in calcium, magnesium, and vitamin D
- seeking preconception counseling if planning pregnancy
If you’re concerned about severe outcomes, you may also want to learn more about Can Graves’ disease kill you and whether Can Graves’ disease be cured. Understanding treatment options and long-term management strategies can provide reassurance and clarity.
The bottom line
Graves’ disease causes hyperthyroidism, and serious complications may develop if thyroid hormone levels remain uncontrolled.
However, with medications, radioactive iodine therapy, or surgery — along with routine follow-up — most individuals achieve stable hormone levels and maintain a normal life expectancy.
If you’re wondering how long you can live with Graves’ disease, the outlook is generally positive when the condition is properly managed. Speak with your doctor to determine the most suitable treatment plan and reduce the risk of long-term complications.





















Leave a Reply
You must be logged in to post a comment.