
Your ear is a sophisticated organ composed of three sections:
- Outer ear: This includes the visible ear and the ear canal, which channels sound waves toward the middle ear.
- Middle ear: Consists of the eardrum and three tiny bones that amplify incoming sound.
- Inner ear: Converts sound waves into electrical impulses sent to the brain. It also houses the vestibular apparatus — structures that inform the brain about balance and spatial orientation.
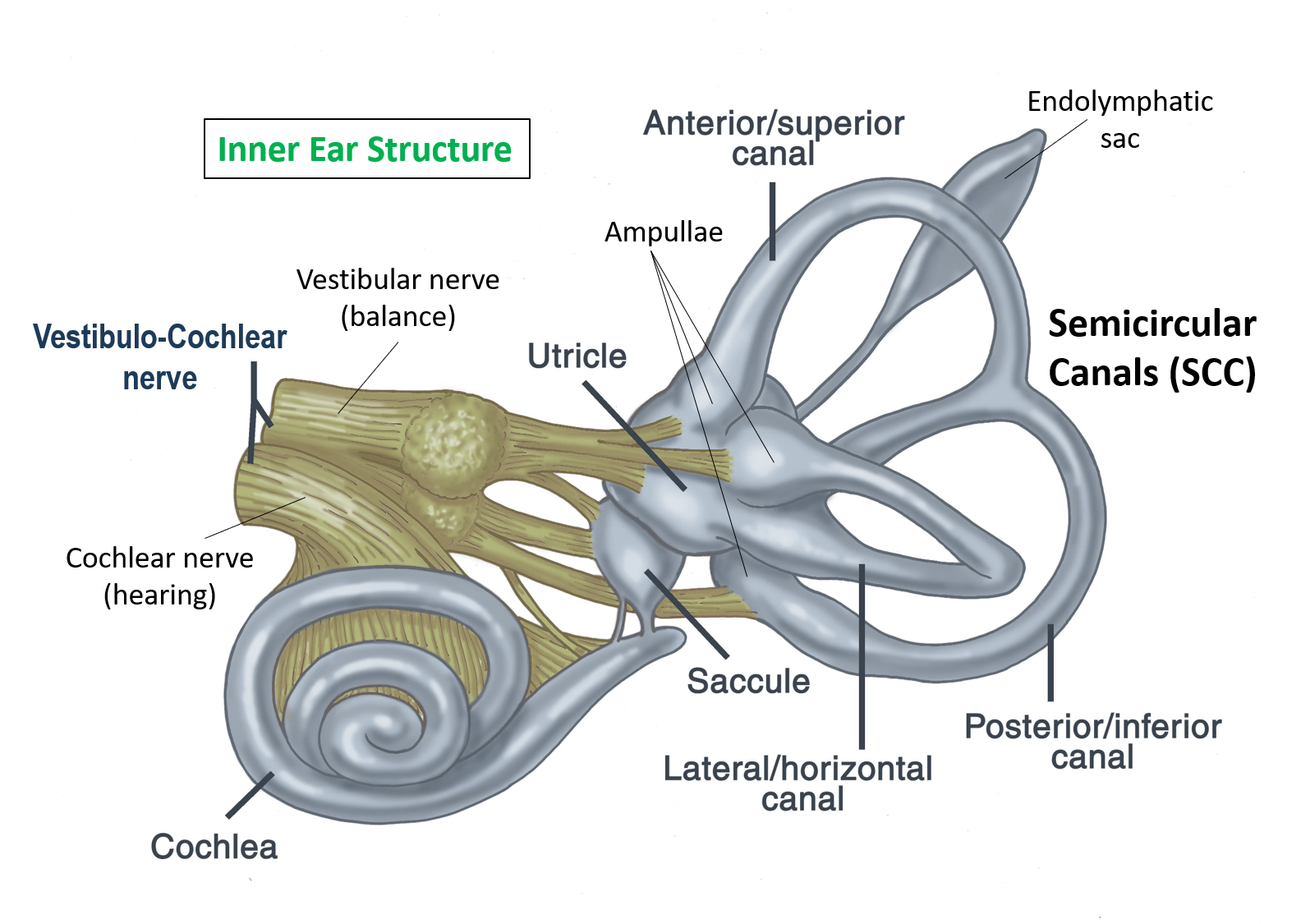
Otoconia, often called ear stones, are minute calcium carbonate crystals located within two vestibular organs known as the saccule and utricle. Typically, otoconia stimulate the hair-like sensory cells of these organs to signal the brain when your body accelerates, as 2015 research describes. This mechanism helps you keep your balance.
Occasionally, otoconia become dislodged from their proper location. When that happens, your sense of balance can be disrupted, leading to a disorder called benign paroxysmal positional vertigo (BPPV).
Below, learn what may cause otoconia problems and how they’re managed.
Why we have ear stones
Everyone has tiny crystals in the inner ear that help the brain interpret motion and changes in speed.
These crystals, otoconia, vary in size from 1 to 30 micrometers (about 1/847 to 1/25,400 of an inch). They’re primarily composed of calcium carbonate — the same material used in calcium supplements and some antacids.
Without otoconia, detecting linear acceleration would be difficult. These crystals press against hair-like cells in the utricle and saccule, stimulating them to send electrical signals to the brain for processing.
The utricle is more responsive to horizontal acceleration, while the saccule is tuned to vertical acceleration. Collectively, these structures are called the otolith organs.
Problems with otoconia can produce balance disturbances and dizziness.
Complications from ear stones
Issues with ear stones are closely linked to a common vestibular disorder called BPPV and may be influenced by age-related changes in balance function.
Benign paroxysmal positional vertigo (BPPV)
Besides the otolith organs, the inner ear contains three semicircular canals filled with fluid. When you move your head, fluid movement bends hair-like cells along the canals’ inner surface, producing signals sent to the brain.
Each semicircular canal has a distinct role:
- One senses forward and backward head motions.
- One detects side-to-side tilt.
- One senses rotational movements of the head.
Otoconia can become detached from the otolith organs and migrate into these semicircular canals, according to experts. When this occurs, it may produce BPPV.
BPPV is the leading cause of vertigo — the false sensation of motion when you are stationary. Vertigo from BPPV tends to be brief and is often triggered by sudden head movements.
Lifetime prevalence of BPPV is estimated at roughly 2.4%, and it appears to be about 2 to 3 times more frequent in women than men.
Age-related loss of otoconia
The vestibular system’s responsiveness decreases with age, though researchers are still determining all the contributing factors.
A 2019 study proposed that age-related loss of otoconia may be a key reason older adults experience poorer balance.
A 2021 review summarized findings suggesting that the number of otoconia in both otolithic organs declines with age, with possibly greater loss in the saccule.
Symptoms of loose ear stones
If otoconia detach and lead to BPPV, common symptoms include:
- dizziness
- lightheadedness
- balance difficulties
- rapid, involuntary eye movements
- nausea and vomiting
When to seek medical care
Contact your healthcare provider if you experience recurrent or unexplained dizziness or vertigo. Dizziness can signal a serious issue. Seek immediate medical attention or visit urgent care if you develop alarming signs such as:
- a new or severe headache
- difficulty speaking or confusion
- double vision
- numbness or tingling in the arms or legs
- loss of consciousness
- falls or sudden collapse
How loose ear stones are diagnosed
BPPV is typically identified through a physical exam that includes the Dix-Hallpike maneuver. This involves a sequence of positions performed in the clinician’s office while the provider observes your responses.
Treatment for loose ear stones
First-line management for BPPV involves physical repositioning techniques designed to move the crystals out of the semicircular canals and back into the otolith organs for reabsorption, according to 2022 research.
These techniques are known as canalith repositioning procedures. The Vestibular Disorders Association reports these maneuvers successfully treat BPPV in around 80% of cases.
Canalith repositioning procedures
The two primary maneuvers used to treat BPPV are the Epley and Semont-Liberatory techniques. The choice depends on the location of the crystals within the ear.
Epley maneuver
In the Epley maneuver, the clinician will typically:
- Turn your head toward the affected ear.
- Have you lie back quickly with your head still turned in that direction.
- Slowly rotate your head in the opposite direction.
- Turn your body so it aligns with your head, with your chin tucked toward the lower shoulder.
- Assist you to sit upright while keeping your head tucked to the shoulder.
- Have you gradually lift your head back up.
This video demonstrates the maneuver.
Semont-Liberatory maneuver
For the Semont-Liberatory maneuver, the practitioner will:
- Seat you on the edge of a bed with your head turned away from the problematic side.
- Swiftly guide you into a side-lying position with your head angled upward.
- Maintain that posture for at least 20 seconds.
- Move you rapidly back up and then onto the opposite side with your head lowered.
- Hold that position for at least 30 seconds.
- Gently return you to a sitting position.
Medications and surgery
Physicians may prescribe medications to relieve dizziness linked to BPPV, such as:
- antihistamines (commonly Meclizine — which eases symptoms but doesn’t fix the root problem)
- anticholinergics
- sedative-hypnotics
In uncommon situations where canalith repositioning fails and BPPV recurs frequently, surgery may be considered. Surgery is performed in under 1% of BPPV cases. Surgical options include:
- Singular neurectomy: Cutting the nerve that transmits signals from the posterior semicircular canal. This can stop vertigo in 80% to 97% of patients but carries a relatively high risk of hearing loss.
- Posterior semicircular canal occlusion: A highly effective procedure in which the surgeon blocks the posterior semicircular canal to reduce abnormal stimulation.
Takeaway
The utricle and saccule in your inner ear contain tiny calcium carbonate crystals called otoconia that let you sense acceleration. If these crystals dislodge and enter the semicircular canals, they can cause BPPV.
BPPV is most often treated with targeted repositioning maneuvers. Surgery is rarely necessary but may be advised for recurrent, severe cases.





















Leave a Reply
You must be logged in to post a comment.