
Neuroendocrine liver cancer arises from cells that release hormones in response to nerve signals. In most instances, neuroendocrine tumors found in the liver have spread from other primary sites.
Liver cancer is responsible for over 700,000 deaths worldwide annually. The predominant form is hepatocellular carcinoma, accounting for roughly 75% of cases.
Neuroendocrine liver cancer is an uncommon form that originates in neuroendocrine cells. Primary neuroendocrine tumors of the liver are exceedingly rare, with only about 200 documented instances.
More commonly, neuroendocrine tumors detected in the liver have metastasized from the gastrointestinal tract or the lungs.
This article explores neuroendocrine liver cancer in greater detail, covering its causes, signs, and available treatment approaches.
What is neuroendocrine liver cancer?
Neuroendocrine tumors develop from neuroendocrine cells, which secrete hormones when stimulated by electrical signals carried by nerves. These cells are dispersed across the body but are most abundant in the digestive system and lungs.
When neuroendocrine cancer originates in the liver it is very uncommon, and clinical experience guiding management is limited. These tumors often grow slowly and are frequently discovered at advanced stages.
In a small number of reports, neuroendocrine liver cancer has been found mixed with hepatocellular carcinoma, the liver’s most prevalent cancer type.
The majority of neuroendocrine liver lesions represent metastases from tumors in the gastrointestinal or respiratory tracts. Liver involvement happens in roughly 27–90% of neuroendocrine tumors arising at other sites.
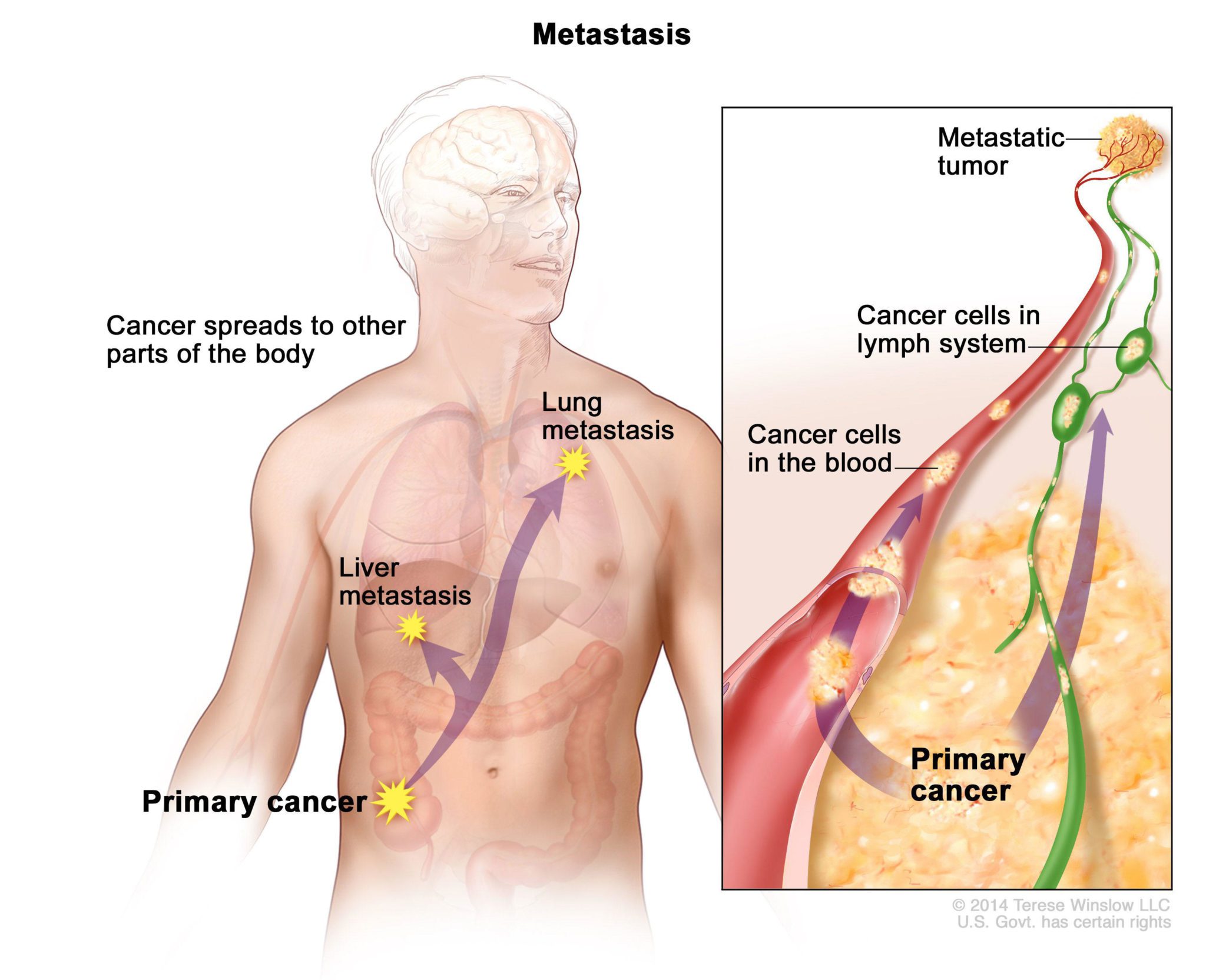
Cancer that has spread from another organ is termed metastasized cancer, commonly classified as stage 4 disease.
What are the symptoms of neuroendocrine liver cancer?
Neuroendocrine liver tumors frequently remain asymptomatic until they attain a substantial size.
As a tumor enlarges, symptoms may include:
- abdominal pain
- abdominal swelling or bloating
- jaundice (yellowing of the skin and eyes)
About 20–30% of neuroendocrine tumors are hormone-producing and provoke systemic symptoms. Tumors that secrete hormones are called functioning tumors.
Functioning tumors can trigger symptom clusters known as paraneoplastic syndromes. In the liver, functioning neuroendocrine tumors can lead to a rare paraneoplastic condition called carcinoid syndrome.
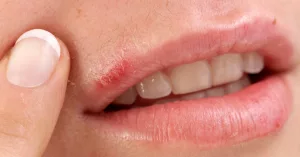
Common manifestations of carcinoid syndrome include:
- flushing of the face and skin
- diarrhea
- reduced appetite
- abdominal discomfort
- fast heart rate
- shortness of breath
- wheezing
What causes neuroendocrine liver cancer and who’s at risk?
Most neuroendocrine tumors found in the liver represent metastatic disease from other body sites. Cancer cells can reach the liver via the bloodstream or the lymphatic system.
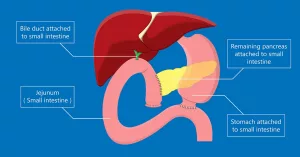
The exact reason why some neuroendocrine tumors might originate in the liver remains unclear. Some experts speculate that ectopic pancreatic tissue—pancreatic cells located outside the pancreas—could be responsible.
Another hypothesis is that these cancers may arise from stem-like cells in the bile duct system within the liver.
The typical age at diagnosis for primary hepatic neuroendocrine tumors is about 47 to 50 years. Few cases are seen under 40, and incidence appears roughly equal between men and women.
How is neuroendocrine liver cancer diagnosed?
Early diagnosis can be challenging because neuroendocrine liver tumors often cause no early symptoms. Common tumor markers like alpha-fetoprotein, useful for other liver cancers, are not reliable for neuroendocrine tumors.
Imaging techniques used to detect neuroendocrine liver tumors include:
- computed tomography (CT) scans
- ultrasound
- magnetic resonance imaging (MRI)
A tissue biopsy can confirm the diagnosis and distinguish neuroendocrine cancer from other tumor types. Biopsy means removing a small sample of tissue for microscopic examination in a lab.
For suspected neuroendocrine liver disease, the specimen is often obtained at the time of surgical removal. Fine-needle biopsy has shown limited accuracy for these tumors.
A biopsy is not required when liver lesions are visible on imaging and there is an established diagnosis of neuroendocrine tumors elsewhere in the body.
How is neuroendocrine liver cancer treated?
Optimal treatment strategies for neuroendocrine liver cancer continue to be defined. When tumors are resectable, curative-intent liver surgery is the preferred approach. However, only about 10–25% of patients with metastatic neuroendocrine liver disease are candidates for surgical cure.
The surgical technique chosen depends on tumor size, number, and location.
Surgical and locoregional options may include:
- partial hepatectomy with removal of adjacent lymph nodes
- total hepatectomy followed by liver transplantation
- selective hepatic artery embolization to cut off the tumor’s blood supply
- radiofrequency ablation to destroy tumor tissue using heat
What’s the outlook for someone with neuroendocrine liver cancer?
Data indicate that among people with primary hepatic neuroendocrine cancer who undergo surgery, about 74% survive at least 5 years, with recurrence occurring in roughly 18%.
A 2021 study found no meaningful difference in survival between patients with small intestine neuroendocrine tumors who did and did not have liver metastases, based on data from 123 individuals. Reported survival rates were:
| Survival time | No spread to liver | Spread to liver |
|---|---|---|
| 1-year | 89.0% | 89.5% |
| 5-year | 68.4% | 69.5% |
| 10-year | 52.8% | 33.2% |
| 20-year | 31.0% | 3.6% |
More favorable outcomes have been observed in patients who undergo intensive treatment, including surgery and liver transplantation. Those who are not candidates for transplant often face worse survival prospects.
Factors that typically preclude eligibility for liver transplantation include:
- cancer spread beyond the liver
- primary cancer in the bile ducts (intrahepatic cholangiocarcinoma)
- a hepatocellular carcinoma larger than 5 cm or more than three tumors larger than 3 cm
- severe cardiac disease
- uncontrolled systemic infection (sepsis)
- active alcohol or substance use disorder
- human immunodeficiency virus infection with AIDS
- nonadherence to recommended care or insufficient social support
- certain anatomical or health-related limitations such as morbid obesity
Takeaway
Neuroendocrine tumors originate in cells that secrete hormones in response to nerve signals. It is very uncommon for these tumors to begin in the liver; most liver neuroendocrine tumors represent metastases from organs like the lungs or gastrointestinal tract.
Research into the most effective treatments is ongoing. At present, surgical removal is regarded as the only potentially curative option.





















Leave a Reply
You must be logged in to post a comment.