
Key takeaways
- Invasive breast cancer develops when malignant cells move beyond their original site in the milk ducts or lobules and grow into nearby breast tissue. The two most frequently diagnosed forms are invasive ductal carcinoma (IDC) and invasive lobular carcinoma (ILC).
- Diagnosis typically requires a combination of clinical breast exams, mammograms, additional imaging studies, biopsies, and blood tests to identify and characterize the cancer. Receptor testing and lymph node biopsies are also performed to determine stage and spread.
- Treatment for invasive breast cancer depends on the stage and biological features of the tumor but often includes surgery, radiation therapy, and systemic treatments such as chemotherapy, targeted therapy, hormone therapy, and immunotherapy.
Breast cancer is the most commonly diagnosed cancer among women in the United States. While many people search for Graphic pictures of breast cancer to better understand how the disease appears, it’s important to recognize that breast cancer is not a single condition. Instead, it includes several distinct subtypes, each with unique characteristics and patterns of growth.
One major category is invasive breast cancer, which occurs when cancer cells extend beyond their point of origin and infiltrate surrounding breast tissue. Viewing Graphic pictures of breast cancer can sometimes help individuals recognize warning signs, but understanding the medical details behind invasive disease is equally essential.

This comprehensive guide explains what invasive breast cancer is, outlines how it’s diagnosed, and reviews the treatment strategies commonly used in clinical practice.
What are the most common types of invasive breast cancer?
The majority of breast cancers are classified as invasive. According to the American Cancer Society, 81% of breast cancer cases fall into this category.
Among invasive cancers, the two most prevalent types are invasive ductal carcinoma and invasive lobular carcinoma.
Invasive ductal carcinoma
Invasive ductal carcinoma (IDC) is the most frequently diagnosed type of breast cancer overall. It accounts for approximately 80% of all invasive breast cancer cases.
IDC originates in the cells that line the milk ducts — the channels responsible for transporting milk from the lobules to the nipple.
With IDC, malignant cells penetrate the duct wall and invade adjacent breast tissue. Over time, these cells may spread to nearby lymph nodes and, in some instances, to distant organs. For visual reference, some individuals review Pictures of breast cancer lumps to understand how IDC-related masses may appear externally or on imaging studies.

Invasive lobular carcinoma
Invasive lobular carcinoma (ILC) is the second most common invasive subtype. About 10% of invasive breast cancers are classified as ILC.
ILC begins in the lobules, the milk-producing glands of the breast. In this condition, cancer cells breach the lobular wall and extend into nearby breast tissue. Similar to IDC, ILC has the potential to metastasize.
Because ILC tends to grow in a single-file pattern and may not form a distinct lump, it can be more difficult to detect with a physical exam or standard mammography. Advanced imaging, such as MRI or reviewing Pictures of breast cancer lumps on ultrasound, may assist in identifying subtle abnormalities. Approximately 1 in 5 individuals with ILC may have cancer present in both breasts.

What are the less common types of invasive breast cancer?
Beyond invasive ductal carcinoma (IDC) and invasive lobular carcinoma (ILC), there are rarer forms of invasive breast cancer, including inflammatory breast cancer and triple-negative breast cancer.
Triple-negative breast cancers can still be IDC or ILC, but they lack estrogen receptors and progesterone receptors and do not overexpress HER2. Because of these biological features, treatment options differ from hormone receptor–positive cancers.
Invasive ductal carcinoma also includes several uncommon subtypes that together account for fewer than 5% of all breast cancers. These classifications are determined by how tumor cells appear under a microscope.
Subtypes of invasive ductal carcinoma include:
- adenoid cystic carcinoma
- medullary carcinoma
- metaplastic carcinoma
- micropapillary carcinoma
- mixed carcinoma
- mucinous carcinoma
- papillary carcinoma
- tubular carcinoma
What are the symptoms of invasive breast cancer?
In some individuals, invasive breast cancer does not produce obvious symptoms initially and may first be identified through routine screening mammography. For others, reviewing Graphic pictures of breast cancer may raise awareness of visual changes that warrant medical evaluation.
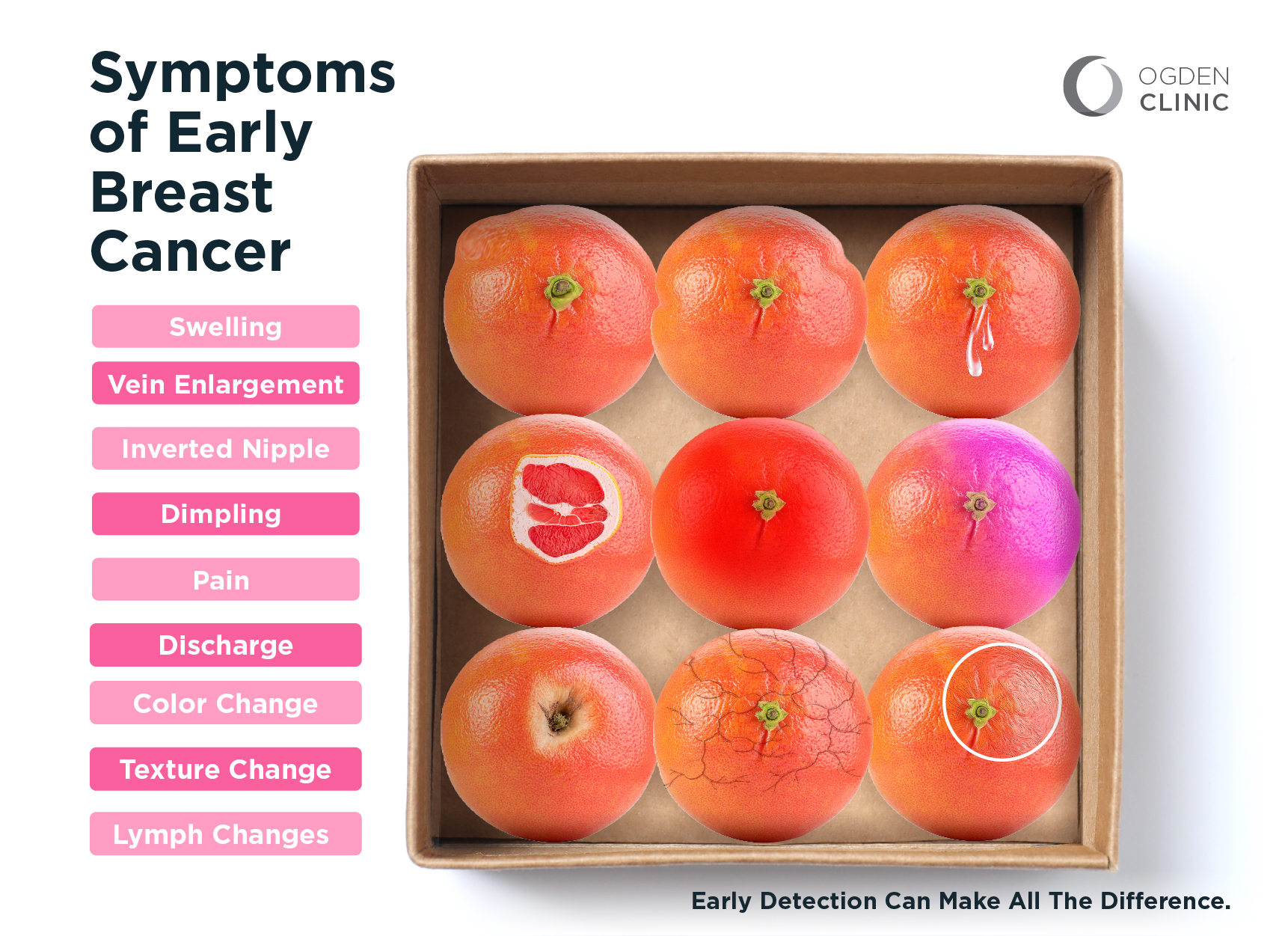
When symptoms do occur, they may include:
- a newly detected lump or area of thickening in the breast or underarm (armpit)
- noticeable alterations in breast size or shape
- skin changes such as redness, swelling, or dimpling (sometimes described as peau d’orange)
- nipple inversion
- discharge from the nipple that is not breastmilk
Any persistent change in breast appearance or texture should prompt consultation with a healthcare professional for further assessment.
How is invasive breast cancer diagnosed?
Diagnosing invasive breast cancer involves multiple diagnostic tools designed to confirm the presence of cancer and define its biological behavior.
- Breast exam: A clinician palpates the breasts and underarm region to detect lumps or structural changes.
- Mammogram: During this imaging test, the breast is compressed between two plates while X-ray images are captured to identify suspicious areas.
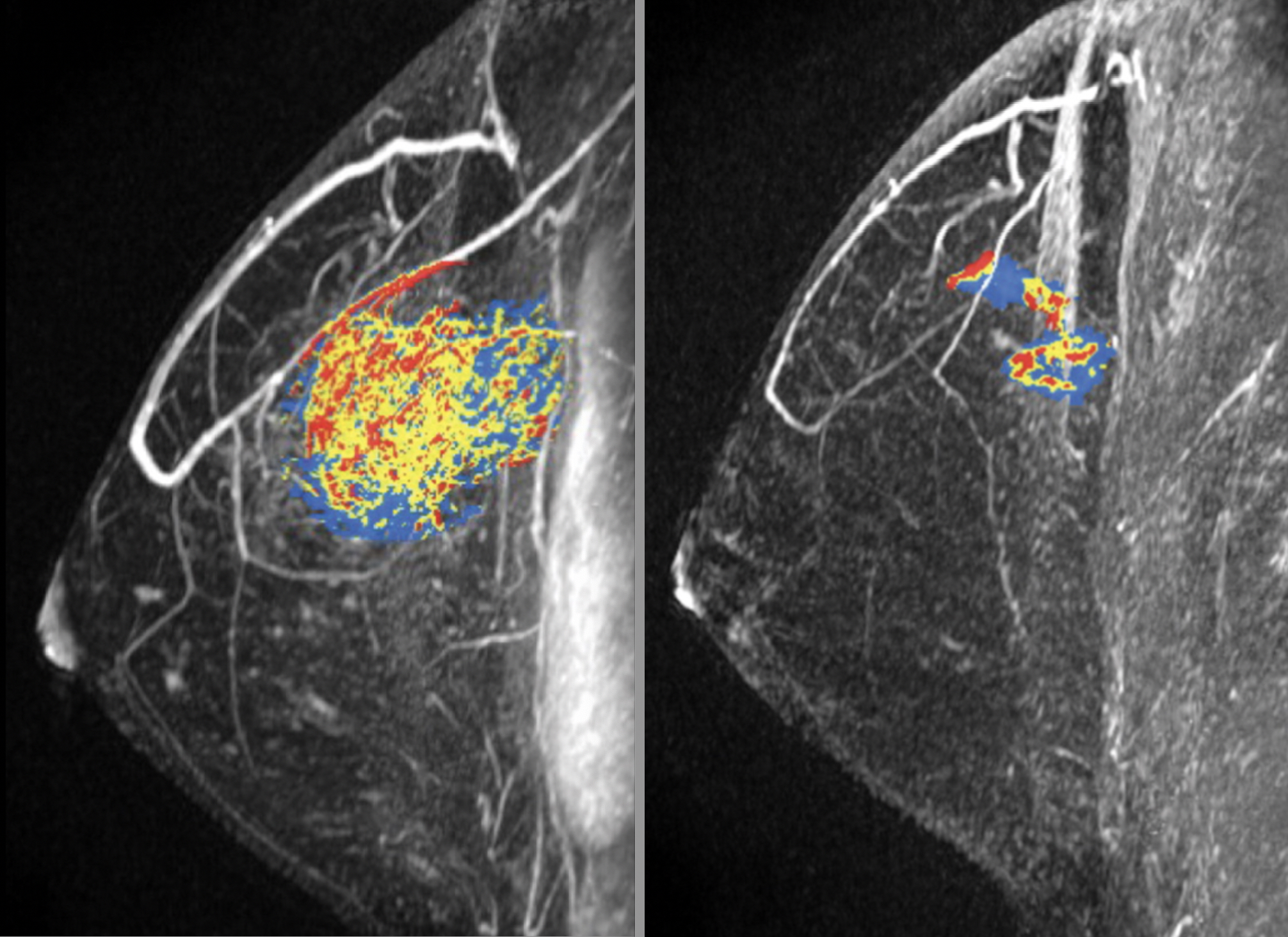
- Imaging tests: Additional imaging, such as ultrasound or magnetic resonance imaging (MRI), may be ordered for further evaluation.
- Biopsy: A tissue sample is removed and examined microscopically to confirm cancer and determine its subtype.
- Blood tests: Blood samples may be analyzed for markers related to overall health and disease status.
If cancer is confirmed, further evaluation helps determine stage and guide treatment planning. These assessments may include:
- Receptor testing: Tests evaluate estrogen receptors, progesterone receptors, and HER2 status.
- Lymph node biopsy: This determines whether cancer has spread to regional lymph nodes.
- Imaging tests: Bone scans, X-rays, CT scans, and positron emission tomography (PET) scans may be used to check for distant metastasis.
How is invasive breast cancer staged?
The presence of invasive cancer cells plays a central role in staging. Cancer confined to its site of origin without invasion into surrounding tissue is referred to as cancer in situ or Stage 0 breast cancer.
Once cancer invades surrounding tissue, it is staged from stage 1 to stage 4, with additional subcategories based on specific findings.
The TNM staging system evaluates:
- Tumor (T): Size of the tumor and extent of local spread
- Lymph nodes (N): Involvement of nearby lymph nodes
- Metastasis (M): Spread to distant organs or tissues
Other influential factors include:
- Tumor grade. Indicates how abnormal the cancer cells appear and how rapidly they may grow and spread.
- HER2 status. Overexpression of human epidermal growth factor receptor 2 (HER2) can accelerate tumor growth.
- Estrogen receptor (ER) status. ER-positive cancers have receptors that bind to estrogen.
- Progesterone receptor (PR) status. PR-positive cancers have receptors that bind to progesterone.
How is invasive breast cancer typically treated?
Treatment decisions depend on stage, receptor status, tumor grade, and overall health. A multidisciplinary oncology team typically develops an individualized treatment plan.
Surgery
Surgery is frequently the first-line treatment for localized invasive breast cancer. It removes the tumor and may also involve lymph node removal.
- Breast-conserving surgery: Also known as lumpectomy or partial mastectomy, this removes the tumor and a margin of surrounding tissue while preserving the breast.
- Total mastectomy: Removal of the entire breast, sometimes including nearby lymph nodes.
- Modified radical mastectomy: Removal of the whole breast, many lymph nodes, and part of the chest lining, occasionally including chest muscle.
Radiation therapy
Radiation therapy delivers high-energy radiation to destroy remaining cancer cells. It may be administered externally or internally (brachytherapy) and is often recommended after surgery to reduce recurrence risk.
Systemic therapies
Systemic therapies circulate through the bloodstream to target cancer cells throughout the body. These treatments may be given orally or intravenously.
- Chemotherapy: Uses potent drugs to inhibit cancer cell growth and division.
- Targeted therapy: Focuses on specific molecular targets associated with cancer cells, minimizing damage to normal tissue.
- Hormone therapy: Blocks hormonal stimulation in ER-positive or PR-positive cancers.
- Immunotherapy: Activates the immune system to attack cancer cells, particularly in some cases of triple negative breast cancer.
Systemic treatments may be administered before surgery (neoadjuvant therapy) to shrink tumors or after surgery (adjuvant therapy) to eliminate residual cancer cells. They are also the primary treatment for metastatic breast cancer.
What’s the difference between invasive and metastatic breast cancer?
Invasive breast cancer refers to cancer that has spread beyond its original structure into surrounding breast tissue. It may remain localized or become metastatic.
If cancer that began in the milk ducts invades nearby breast tissue but does not spread elsewhere, it is invasive but not metastatic.
When cancer cells travel to distant organs such as the liver or lungs, the disease is classified as metastatic. In that situation, the breast cancer is both invasive and metastatic.
What’s the outlook for someone with invasive breast cancer?
Relative survival rates estimate the proportion of individuals alive 5 years after diagnosis compared to those without breast cancer.
Based on the SEER database from the National Cancer Institute (NCI), 5-year relative survival rates are:
| Cancer location/spread | 5-year relative survival rate |
| Localized (cancer remains localized to the breast) | 99% |
| Regional (cancer has spread to lymph nodes or to nearby tissues) | 86% |
| Distant (cancer has spread to more distant tissues of the body | 31% |
| All types combined | 90% |
These statistics reflect women diagnosed between 2013 and 2019. While helpful for understanding overall trends, they cannot predict individual outcomes. Age, general health, tumor biology, and access to modern therapies all influence prognosis. Continued advances in targeted therapy, hormone therapy, and immunotherapy are steadily improving survival rates.
Breast cancer support
A diagnosis of invasive breast cancer can affect physical, emotional, and psychological well-being. Support networks and educational resources can play a vital role in coping and recovery.
- The Breast Cancer HealthEH app connects individuals with a supportive community. Through the HealthEH app, users can interact with others who share similar experiences. Download it here.
- The American Cancer Society offers a variety of services, including a 24/7 helpline (800-227-2345) and transportation assistance.
- Breastcancer.org provides educational resources, discussion boards, and podcasts.
- Living Beyond Breast Cancer (LBBC) delivers support services and opportunities to connect with others.
- The Centers for Disease Control and Prevention (CDC) provides access to low-cost screenings and educational videos.
Takeaway
Invasive breast cancer occurs when malignant cells spread beyond their original location into healthy breast tissue. It may remain confined to the breast or progress to distant organs.
The most common forms are invasive ductal carcinoma and invasive lobular carcinoma, though less common variants exist. Early detection — whether through screening, clinical evaluation, or careful attention to physical changes — significantly improves outcomes.
If you notice unusual breast symptoms or changes similar to those seen in Graphic pictures of breast cancer, schedule an appointment with a qualified healthcare professional. Prompt evaluation and appropriate treatment offer the best chance for successful management.






















Leave a Reply
You must be logged in to post a comment.