
Key takeaways
- Graves’ disease is an autoimmune disorder that results in hyperthyroidism and may impact the heart, eyes, muscles, and bones. It affects about 1.2% of people in the United States.
- Life expectancy is closely tied to how effectively thyroid function is regulated, typically monitored using thyroid-stimulating hormone (TSH) levels. Persistently low TSH is associated with an increased risk of death and more cardiovascular events.
- Graves’ disease can relapse even during treatment, and roughly half of individuals need a treatment adjustment within 12 to 18 months. While therapies can relieve symptoms, they are often not “curative,” and some may result in hypothyroidism.
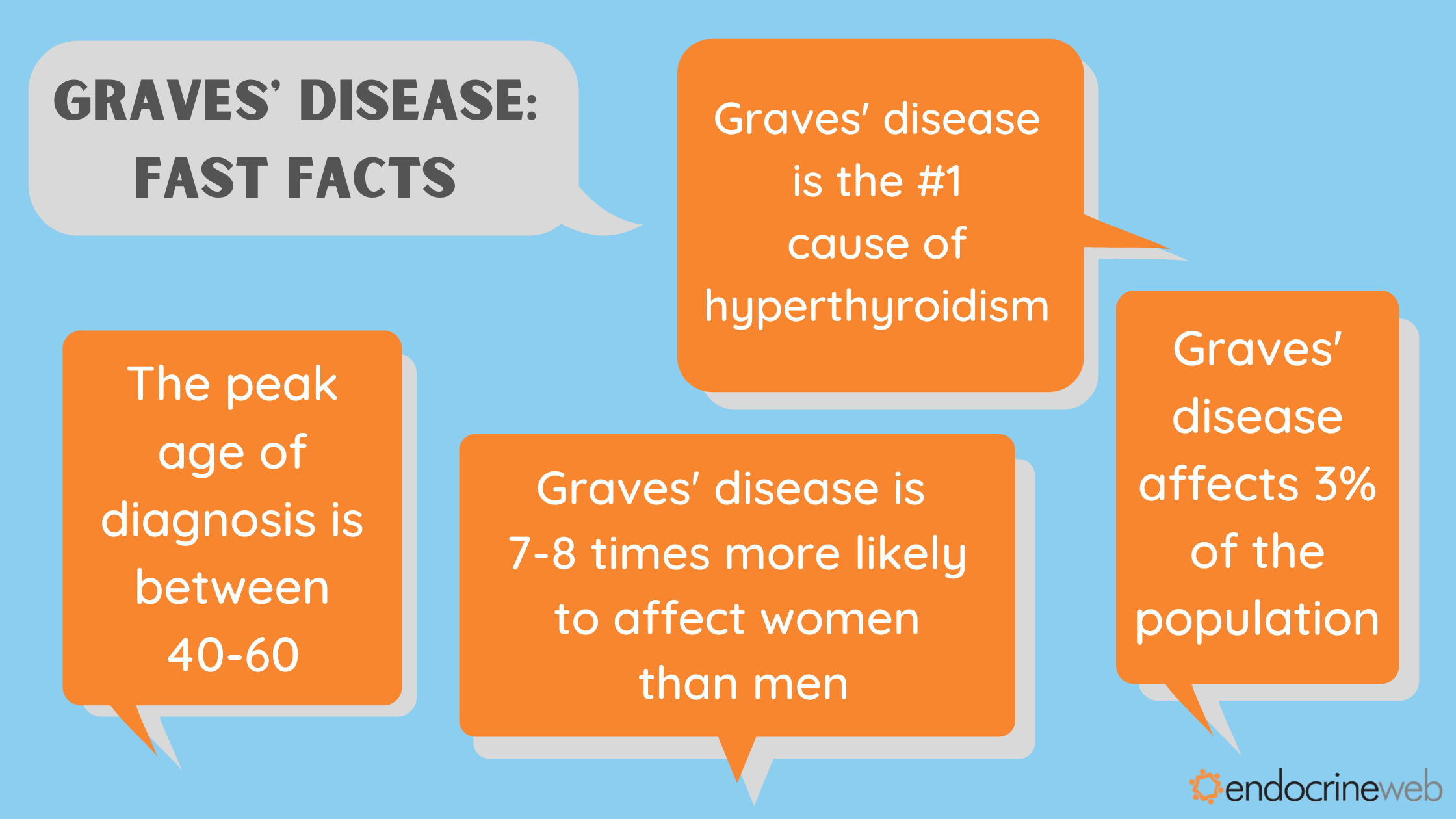
Graves’ disease is an autoimmune condition that overstimulates the thyroid gland, leading to hyperthyroidism. It affects approximately 1.2% of people in the United States and occurs most frequently in women and adults between 20 and 50 years of age.
The thyroid produces hormones that regulate metabolism and influence nearly every organ system. When thyroid hormone levels become excessive, the consequences can extend to the cardiovascular system, muscles, skeletal health, and even the eyes. Because of these widespread effects, many people are understandably concerned about the Life expectancy of someone with Graves’ disease and how the condition may shape their long-term health outlook.
Below, we address common questions about prognosis, daily functioning, and what living with Graves’ disease may mean for your future well-being.
What is the life expectancy for someone with Graves’ disease?
Graves’ disease can trigger systemic changes that raise the risk of serious complications, some of which may be life-threatening. Cardiovascular complications are among the most significant concerns.
The Life expectancy of someone with Graves’ disease largely depends on how well thyroid hormone levels are brought under control. Clinicians typically evaluate this using thyroid-stimulating hormone (TSH) levels, which are usually suppressed (lower than normal) in people with active Graves’ disease.
Low TSH levels reflect the body’s response to excessive thyroid hormone production. When TSH remains persistently low, it signals ongoing thyroid overactivity.
Research examining the relationship between thyroid function and mortality in Graves’ disease has shown that suppressed TSH levels are linked to a higher risk of death — increasing mortality by more than 10% within 6 months of diagnosis, according to one study.
The longer thyroid function stays uncontrolled, the greater the danger. After 5 years of persistently low TSH, individuals were found to be more than twice as likely to die early.
Cardiovascular disease is the leading cause of premature death in people with hyperthyroidism and is strongly influenced by thyroid hormone levels. In another study, the risk of events such as heart attack, arrhythmia, or stroke was significantly elevated.
Even in individuals whose thyroid levels fall within the “normal” reference range, those with relatively higher thyroid activity were found to live about 3 years less than people with lower thyroid activity.
A long-term analysis of 182 individuals with Graves’ disease found that more than one-third achieved normal thyroid function, while 13% developed hypothyroidism following antithyroid therapy. Over 25 years of follow-up, 25 participants died at a median age of 74 years, with cancer being the most common cause of death.
These findings highlight that early diagnosis, consistent monitoring, and appropriate treatment significantly influence the long-term prognosis and overall survival outcomes.
Is Graves’ disease a permanent disability?
For some individuals, Graves’ disease may result in complications that cause lasting impairment, including vision loss from Graves’ orbitopathy, chronic pain, or heart-related issues.
With timely and effective treatment, many of these complications can be prevented or managed. However, research indicates that up to 18% of people required long-term sick leave or permanent disability benefits due to the impact of their condition.
The degree of disability often depends on how quickly hyperthyroidism is controlled and whether complications are addressed early. Regular endocrinology follow-up and lifestyle adjustments can reduce long-term limitations.
What is the quality of life for someone with Graves’ disease?
Quality of life in Graves’ disease varies and is influenced by symptom severity, treatment approach, and whether hypothyroidism develops after therapy. Reduced quality of life has been most strongly linked to post-treatment hypothyroidism.
An older study found that individuals treated with radioiodine therapy reported lower self-rated quality of life compared with those who received antithyroid drugs such as methimazole or propylthiouracil or underwent surgical thyroidectomy.
This suggests that long-term antithyroid drug therapy may preserve quality of life better than treatments that result in permanent hypothyroidism. That said, uncontrolled hyperthyroidism can cause serious complications, and hypothyroidism is typically more straightforward to manage with thyroid hormone replacement.
Many patients share personal experiences about how the condition affects daily living, including stories like Graves’ disease ruined my life, while others discuss recovery journeys such as I cured my Graves’ disease. These narratives highlight the variability of individual outcomes.
When evaluating treatment options, it’s essential to have an open discussion with your healthcare provider about symptom control, emotional well-being, long-term monitoring, and how each therapy may influence your overall lifestyle.
What causes Graves’ disease to flare up?
Graves’ disease can relapse, even after initial improvement with therapy. It is estimated that about half of individuals experience recurrence and may need a change in treatment within 12 to 18 months of starting medication.
Certain risk factors are associated with relapse after antithyroid drug therapy. Some, such as age or male sex, are not modifiable. Smoking has been identified as a predictor of poorer treatment response, making smoking cessation an important preventive strategy.
Graves’ orbitopathy may worsen with uncontrolled thyroid hormone levels and has also been associated with radioiodine therapy. Preventive measures, including oral steroids and antioxidants, may be recommended to reduce the likelihood of eye complications.
Maintaining consistent follow-up appointments, adhering to prescribed medications, and promptly addressing symptom changes can help reduce the risk of flare-ups.
Can you reverse Graves’ disease?
Treatment strategies for Graves’ disease focus on lowering thyroid hormone levels and relieving symptoms of hyperthyroidism. However, they do not eliminate the underlying autoimmune process responsible for the condition.
Surgical thyroidectomy or radioiodine therapy can significantly reduce or eliminate thyroid activity, but these approaches commonly result in hypothyroidism, requiring lifelong thyroid hormone replacement. For this reason, Graves’ disease is generally not considered “curable.”
Nevertheless, about one-third of individuals may achieve normal thyroid hormone levels with treatment, and remission has been reported in more than a quarter of cases.
Long-term remission is more likely when thyroid levels are stabilized early and monitored regularly, reinforcing the importance of individualized care plans.
The takeaway
Graves’ disease is a chronic autoimmune disorder that causes elevated thyroid hormone levels and can influence multiple organ systems.
If not properly managed, hyperthyroidism may lead to complications such as cardiovascular disease, eye disorders, and increased mortality risk. The Life expectancy of someone with Graves’ disease is closely tied to how effectively thyroid function is controlled over time.
Available treatments — including antithyroid medications, radioiodine therapy, and surgery — can restore hormone balance and lower the risk of complications, though each approach carries specific considerations.
Before initiating or changing treatment, discuss the potential benefits, risks, and long-term implications with your doctor, including how each option may affect your quality of life and overall health trajectory.


















Leave a Reply
You must be logged in to post a comment.