Imagine you’ve been waking up with stubborn joint stiffness, a lingering ache in your wrists, and a fatigue that just won’t quit. You’ve Googled “why am I so sore” and landed on a page that promises the answer in three simple steps. Spoiler: it’s not magic, but it is doable—if you know what doctors look for.
In the next few minutes, I’ll walk you through exactly how a rheumatologist puts the puzzle pieces together for a rheumatoid arthritis diagnosis. We’ll cover the symptoms that raise red flags, the blood work (the infamous RA blood tests), the imaging tricks that reveal hidden inflammation, and the scoring system that decides whether you truly have RA. By the end, you’ll feel empowered to ask the right questions at your next appointment and, most importantly, understand why catching RA early can be a game‑changer for your joints and your life.
Understanding the Diagnostic Journey
Getting a diagnosis isn’t usually a one‑stop shop. Think of it as a short road trip with a few checkpoints—each one builds the case for RA.
First stop: Symptom check‑in
When you first see a doctor, the conversation centers on what you’ve been feeling. Details matter: How long have the joints been swollen? Which joints are involved? Does the pain improve after you start moving, or does it linger? A thorough history helps the clinician differentiate rheumatoid arthritis from other forms of arthritis that might masquerade in the same way.
Second stop: Referral to a specialist
Primary‑care physicians can order initial labs, but the gold standard for confirming RA is a rheumatologist. These specialists have “physician expertise” that according to Arthritis‑Health, makes them comfortable recognizing subtle patterns that point to RA versus, say, psoriatic arthritis or lupus.
Third stop: Timeline expectations
Most people hear back within 2–4 weeks after the first blood draw. If imaging is required, add another week or two. In practice, many patients report a total journey of 6–12 weeks from the first visit to a firm diagnosis. Patience is key—early detection still beats waiting until the disease has “settled in.”
Core Symptoms to Watch
RA loves symmetry. That’s a fancy way of saying it usually attacks the same joints on both sides of the body. Keep an eye out for these tell‑tale signs:
Symmetrical joint swelling
Look at your wrists, knuckles (the MCP and PIP joints), and the small joints of your feet. Swelling that mirrors itself on the left and right is classic RA.
Morning stiffness that outlasts coffee
If you’re still feeling stiff after 30 minutes of gentle movement, it’s a red flag. In osteoarthritis, stiffness typically eases within 15 minutes.
Systemic clues
Fatigue, low‑grade fever, and a general sense of “not feeling well” often accompany the joint pain. These “systemic” symptoms happen because RA is an inflammatory disease that can affect the whole body—not just the joints.
Red‑flag extras
Rapidly progressive swelling, rheumatoid nodules under the skin, or unexplained weight loss should prompt an urgent visit. These may signal aggressive disease that needs immediate treatment.
Essential RA Blood Tests
There’s no single “RA test” that guarantees a diagnosis, but a panel of blood work paints a pretty reliable picture. Let’s break down the most common ones.
Rheumatoid factor (RF)
RF is an antibody that targets the body’s own tissue. About 70‑80 % of established RA patients have a positive RF, but remember it’s not exclusive to RA—people with hepatitis C or even healthy folks can test positive.
Anti‑CCP (anti‑cyclic citrullinated peptide) antibodies
Anti‑CCP is the superstar of RA testing. It’s highly specific: a positive result strongly suggests RA, and it can appear even before symptoms flare. According to the NHS, anti‑CCP is present in 60‑80 % of people with RA and predicts a more aggressive disease course.
Acute‑phase reactants: ESR & CRP
These tests measure how inflamed your body is. The erythrocyte sedimentation rate (ESR) looks at how quickly red blood cells settle, while C‑reactive protein (CRP) quantifies a protein the liver pumps out during inflammation. Both are useful for tracking disease activity, even if they’re not diagnostic on their own.
Full blood count & ANA
A complete blood count can reveal anemia, which occurs in many RA patients, and help rule out other causes of fatigue. Antinuclear antibody (ANA) testing is broader, flagging autoimmunity in general; a positive ANA doesn’t confirm RA but may point the clinician toward other autoimmune disorders.
| Test | Sensitivity | Specificity | What It Shows |
|---|---|---|---|
| RF | ≈ 70 % | ≈ 85 % | Autoantibody; can be positive in other diseases |
| Anti‑CCP | ≈ 80 % | ≈ 95 % | Highly specific for RA; predicts erosive disease |
| ESR | Variable | Low | General inflammation marker |
| CRP | Variable | Low | Acute inflammation marker |
Imaging That Helps Diagnose
When blood work points toward RA but you need visual confirmation, imaging steps in. Each modality offers a different window into your joints.
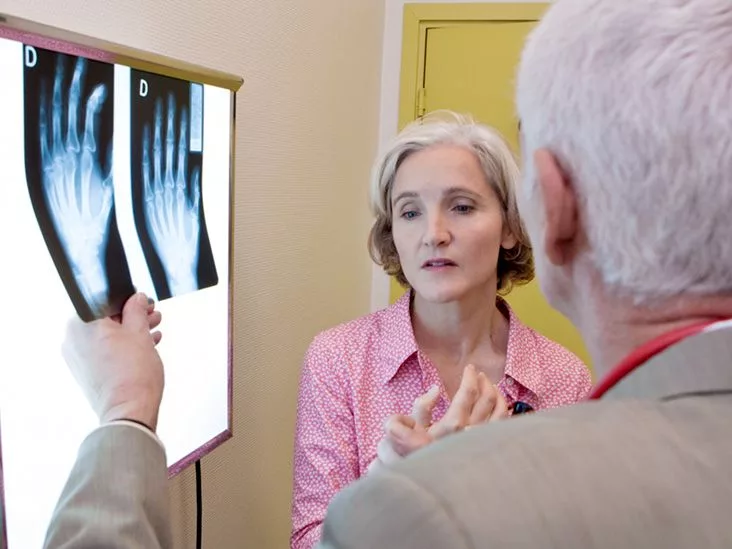
X‑ray – the classic start
X‑rays reveal bone erosion and joint space narrowing—hallmarks of later‑stage RA. However, in early disease the X‑ray can look perfectly normal, which is why doctors often move on to more sensitive tools.
Ultrasound – “the feel‑good” scan
Ultrasound lets the clinician see synovial thickening (inflammation of the joint lining) and tiny fluid collections that are invisible on X‑ray. It’s quick, inexpensive, and especially useful for early detection.
MRI – the deep dive
MRI is the most sensitive imaging for early RA. It shows bone‑marrow edema, subtle erosions, and inflammation of the tendons. The downside? Higher cost and limited availability, so it’s usually reserved for ambiguous cases.
| Modality | Best For | Cost | Availability |
|---|---|---|---|
| X‑ray | Bone erosion, joint space loss | Low | Widely available |
| Ultrasound | Synovitis, effusion | Moderate | Growing in clinics |
| MRI | Early erosions, bone‑marrow edema | High | Specialized centers |
Classification Criteria Explained
The 2010 ACR/EULAR classification criteria act like a scoring chart. Doctors assign points for four domains: joint involvement, serology, acute‑phase reactants, and symptom duration. Reach 6 or more points, and the diagnosis of RA is highly likely.
Scoring snapshot
- Joint involvement: 0–5 points (more points for multiple small joints).
- Serology: 0–3 points (positive RF or anti‑CCP adds points).
- Acute‑phase reactants: 0 or 1 point (elevated ESR/CRP).
- Symptom duration: 0 or 1 point (≥ 6 weeks adds a point).
Imagine a patient with swelling in three small joints (2 points), a positive anti‑CCP (2 points), elevated CRP (1 point), and symptoms for 8 weeks (1 point). That totals 6 points—crossing the threshold for a rheumatoid arthritis diagnosis.
Undifferentiated Arthritis Insight
Not every joint pain fits neatly into the RA box. When a patient doesn’t meet the full criteria, doctors may label the condition “undifferentiated arthritis.” Roughly one‑third of these cases evolve into full‑blown RA, another third resolve or turn out to be a different disease, and the remaining stay ambiguous.
Why does this matter? Early, low‑dose DMARD (disease‑modifying anti‑rheumatic drug) therapy can sometimes halt progression, even when the diagnosis isn’t crystal clear yet. That’s why clinicians keep a close eye on the “gray zone” and repeat labs and imaging every few months.
Weighing Benefits and Risks
Deciding to start treatment before the disease is fully confirmed feels like a gamble. Let’s lay out the pros and cons.
Benefits of early diagnosis
- Prevents irreversible joint erosion.
- Increases the chance of achieving remission with first‑line DMARDs.
- Reduces systemic complications (cardiovascular disease, osteoporosis).
Potential risks
- Exposure to immunosuppressive meds that can increase infection risk.
- Side‑effects such as liver toxicity or gastrointestinal upset.
- Psychological impact of a chronic disease label.
The sweet spot is shared decision‑making: you, your rheumatologist, and any supportive loved ones weigh the evidence together. A gentle, transparent conversation helps you feel confident about the chosen path.
Real‑World Patient Stories
Stories bring data to life. Here are two concise snapshots that illustrate the journey.
Emma’s early hunt
Emma, 28, first noticed stiffness in her fingers after a weekend of hiking. She thought it was “just sore muscles.” After three months of lingering pain, her GP ordered RF and anti‑CCP. RF was negative, but anti‑CCP came back strongly positive. An ultrasound showed synovitis, and within weeks she started methotrexate. Six months later, her disease activity score dropped from 6.5 to 2.1, and she’s back to rock‑climbing.
James’s undifferentiated path
James, 45, presented with swelling in one knee and two wrists. Labs were inconclusive, and X‑rays were normal. The rheumatologist diagnosed “undifferentiated arthritis” and started a low‑dose DMARD while scheduling repeat labs in three months. By the next visit, anti‑CCP turned positive and his score hit 7 points on the ACR/EULAR chart—confirming RA. Early treatment meant he avoided any joint damage visible on later X‑rays.
Practical Action Steps
Now that you’ve got the roadmap, here’s a simple checklist to bring to your next appointment:
- Symptom diary: Write down which joints hurt, when stiffness starts, and how long it lasts.
- Family history note: Mention any relatives with RA, lupus, or other autoimmune diseases.
- Medication list: Include over‑the‑counter drugs and supplements—some can affect blood test results.
- Questions to ask:
- “Would anti‑CCP be useful for me right now?”
- “If my RF is negative, can we still confirm RA?”
- “What imaging would you recommend based on my symptoms?”
- Downloadable tracker: (Consider creating a PDF “RA Diagnosis Tracker” for yourself.)
Remember, you’re the partner in this diagnostic dance. The more precise the information you give, the faster the doctor can move from “maybe” to “definitely” and start the treatment that protects your joints.
Conclusion
Getting a rheumatoid arthritis diagnosis is a blend of careful listening, targeted lab work, and the right imaging—all tied together by a scoring system that helps clinicians feel confident. Early detection isn’t just about starting medication sooner; it’s about preserving the life you love—whether that’s dancing, gardening, or simply playing with the grandchildren without pain.
If you recognize any of the symptoms described, don’t wait. Schedule that appointment, bring your symptom diary, and ask about the anti‑CCP test. You deserve clear answers and a treatment plan that puts you back in control.
Got questions or a personal story you’d like to share? Drop a comment below or reach out to your healthcare team. We’re all in this together, and every step you take brings you closer to feeling your best.




















Leave a Reply
You must be logged in to post a comment.