
Bottom‑surgery healing is a journey, not a race. Most folks wonder how long it takes to see a “healed” result, whether the scar will ever fade, and what they can do every day to make the process smoother. Below you’ll find a friendly, step‑by‑step guide that tackles those questions head‑on, sprinkled with real‑world tips, expert insights, and a dash of humor to keep things light.
Quick Answer
In general, the wound from a bottom surgery is considered fully healed after 4 – 6 months of proper care, while the scar can keep remodeling for up to a year. The exact timeline depends on two big factors: the type of procedure you had (vaginoplasty, phalloplasty, etc.) and how diligently you follow post‑op instructions.
Think of it like learning to ride a bike again after a fall—you’ll be able to pedal after a few weeks, but mastering smooth turns takes a bit longer. Below we’ll break down each “type of bike” and the road you’ll travel on.
Surgery Types
Feminizing (MTF) Surgery
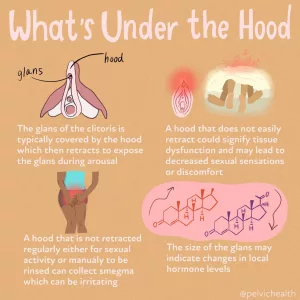
When we talk about “mtf bottom surgery” most people are referring to vaginoplasty (full‑depth) or vulvoplasty (zero‑depth). The surgeon creates a vaginal canal, labia, clitoral hood, and clitoris using penile and scrotal tissue. Healing centers around two main zones: the external vulvar incisions and the internal canal.
Cleveland Clinic notes that the external scars usually soften within three months, while the internal canal continues to epithelialize (grow new lining) for up to six months. During that time, dilation is key to prevent narrowing.
Typical healed appearance
- Labia look like natural folds, with a faint line where the incision was made.
- The neovaginal depth stabilizes around 4‑6 cm and feels similar to natal vaginal tissue after several months of regular dilation.
- Scars may be barely visible, especially if silicone sheets were used.
Masculinizing (FTM) Surgery
For trans men, “bottom surgery” often means either phalloplasty (building a neophallus from a flap of tissue) or metoidioplasty (elongating the existing clitoris). Both involve urethral lengthening, which adds a layer of complexity to healing.
Phalloplasty patients usually have multiple donor‑site scars (forearm, thigh, or abdomen) and a primary penile shaft scar. Metoidioplasty results in a smaller external scar but still requires careful urethral care.
Typical healed outcome
- The neophallus becomes pliable enough for sexual activity after 3‑6 months.
- Urethral healing is considered complete when there’s no leaking or stricture—often verified at the 2‑month follow‑up.
- Donor‑site scars fade like any other surgical scar, especially with silicone therapy.
Partial or Hybrid Procedures
Procedures such as orchiectomy, scrotectomy, or penectomy are less extensive but still have a healing curve. Because the incisions are smaller, “full healing” often occurs in 4‑8 weeks, yet scar care remains important, especially for individuals with darker skin tones who may be prone to keloids.
Healing Timeline
| Phase | Typical Duration | What’s Happening Inside | Key Care Tasks |
|---|---|---|---|
| Immediate Post‑Op (0‑7 days) | 1 week | Inflammation, clot formation, catheter placement for many patients | Keep dressings dry, monitor urine output, take prescribed pain meds, avoid strenuous movement |
| Early Healing (1‑4 weeks) | Up to 1 month | Granulation tissue fills the wound; sutures start to dissolve | Start gentle dilations (if applicable), wash with warm soapy water twice daily, watch for excessive granulation |
| Mid‑Recovery (1‑3 months) | 1‑3 months | Collagen remodeling; scar begins to soften | Apply silicone sheets, massage scar in direction of fibers, protect from sun, maintain hydration |
| Late Recovery (3‑12 months) | 3‑12 months | Scar maturation (type II‑III collagen); keloid risk wanes | Continue silicone therapy, avoid smoking, schedule final clearance visits |
Those four blocks give you a mental map of what to expect. If you’re the type who loves a checklist, copy this table into a note and tick off each task as you go. Trust me— watching the “progress bar” fill up is oddly satisfying.
Common Issues
Granulation Tissue
Ever seen a piece of raw, bright‑red “ground beef” after a surgery? That’s granulation tissue, and it’s a normal part of secondary‑intention healing (the body fills the wound from the bottom up). It can be tender, especially around the vaginal canal or urethral site.
According to QueerDoc, treatments include:
- Applying silver nitrate by a clinician to gently cauterize excess tissue.
- Medical‑grade honey (e.g., Medihoney) applied to the area to reduce inflammation.
- Low‑strength topical steroids (triamcinolone) if the tissue refuses to shrink.
If granulation persists beyond two weeks or is unusually painful, give your surgeon a call—early intervention prevents longer downtime.
Scars and Their Types
Scars aren’t one‑size‑fits‑all. Here’s a quick rundown:
- Cicatrix – the “normal” thin line that fades over time.
- Hypertrophic – raised but stays inside the incision border.
- Keloid – spreads beyond the original cut; more common in darker skin tones.
- Contracture – tight scar that can restrict movement.
Managing Your Scars
- Silicone therapy: Apply silicone sheets or tape for 12 hours a day (start after the stitches are gone). This is the gold‑standard for flattening hypertrophic and keloid scars.
- Massage: Gently rub the scar in the direction of the line for 2‑3 minutes, twice daily. It encourages collagen realignment.
- Sun protection: UV rays darken scars. A broad‑spectrum SPF 30+ can cut hyperpigmentation in half.
- Quit smoking: The RSA blog points out that tobacco reduces oxygen to healing tissue, lengthening scar maturation and increasing infection risk.
Infection & Catheter Care
Most infections show up as redness, swelling, foul odor, or fever. Keep the area clean with a mild wound cleanser and warm saline rinse twice a day. For those with a catheter, use alcohol pads to sterilize the connections (see the same QueerDoc article for a step‑by‑step). If you notice any pus, increasing pain, or a temperature over 100.4 °F, reach out to your surgeon immediately.
Physical Comfort Aids
Simple tricks make a world of difference:
- Wear a donut cushion when you sit to relieve pressure on the perineum.
- Choose slip‑on shoes (no laces) to avoid bending that could strain incisions.
- Use a bending straw for drinks or meds—no need to lean forward and tug at the stitches.
- Keep an ice pack (20 minutes on, 20 minutes off) handy for sudden swelling spikes.
Lifestyle Tips
| Factor | Why It Matters | Practical Tip |
|---|---|---|
| Quit smoking | Improves oxygen delivery and collagen synthesis | Use nicotine patches or gum at least two months before surgery |
| Maintain healthy weight | Reduces tension on sutures and promotes circulation | Light cardio + protein‑rich meals for three weeks pre‑op |
| Stay hydrated | Supports tissue regeneration | Drink 2–3 L of water daily; add electrolytes if you’re active |
| Pelvic‑floor exercises | Boosts blood flow, eases swelling | After clearance, do gentle Kegels 5 × 10 seconds each day |
| Avoid prolonged sitting | Prevents pressure on incisions that can delay healing | Stand or walk 5 minutes every hour; set a timer |
These aren’t “diet plans” or “gym regimes.” Think of them as little daily habits that add up to a smoother recovery. Even a simple walk around the block can boost circulation and lift your mood.
Cost Overview
Typical Price Ranges (U.S.)
- Feminizing vaginoplasty: $30 k – $50 k
- Masculinizing phalloplasty: $50 k – $100 k
- Metodiaplasty or orchiectomy: $8 k – $20 k
What’s Included?
When you receive a quote, it usually bundles the surgeon’s fee, anesthesia, hospital or ASC fees, post‑op garments, dilators or stents, and follow‑up visits. Some clinics also include scar‑care kits (silicone sheets, saline wipes) as part of the package.
Insurance Navigation
Most insurers recognize CPT codes 54400 (vaginoplasty) and 54390 (phalloplasty) as medically necessary for gender‑affirming care. Your best bet is to obtain a Letter of Medical Necessity from your endocrinologist and attach it to a pre‑authorization request. If you hit a denial, consider an appeal—many patients succeed on the second or third try.
According to the American Society of Plastic Surgeons, the average out‑of‑pocket cost after insurance can still be several thousand dollars, so budgeting early (or exploring financing plans offered by many gender‑affirming centers) is wise.
Expert & Community Resources
Below are a few trustworthy places where you can dig deeper or ask specific questions:
- Cleveland Clinic – detailed procedural overviews and recovery tips.
- QueerDoc – clear explanations of granulation tissue and wound care.
- RSA Docs – deep dive into scar types and management.
- Local LGBTQ+ health centers – many offer support groups where you can share experiences with people who truly understand the ups and downs.
- World Professional Association for Transgender Health (WPATH) – guidelines on hormone‑surgery coordination.
When you reach out to a professional, bring a list of questions. It not only shows you’re prepared but also helps the clinician tailor advice to your anatomy and lifestyle.
Conclusion
Healing after bottom surgery is a blend of biology, attentive care, and a pinch of patience. By knowing the typical timeline, anticipating common bumps like granulation tissue or stubborn scars, and embracing lifestyle habits that boost circulation, you give your body the best shot at a smooth, beautiful result.
Remember: every scar tells a story, and every healed wound marks a step toward living authentically in your own skin. If you’re preparing for surgery, start gathering your post‑op kit now; if you’re already on the road to recovery, celebrate each tiny milestone—whether it’s a scar that’s less pink today or a week of pain‑free dilations.
What part of the healing journey feels most daunting to you? Drop a comment, share your own tip, or ask a question. We’re all in this together, and your experience could be the exact piece of advice someone else needs right now.




















Leave a Reply
You must be logged in to post a comment.